J Korean Ophthalmol Soc.
2017 Feb;58(2):235-239. 10.3341/jkos.2017.58.2.235.
A Case of Immediate Surgical Repair in Traumatic Isolated Inferior Rectus Muscle Rupture
- Affiliations
-
- 1Department of Ophthalmology, Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. Limkh@ewha.ac.kr
- KMID: 2369476
- DOI: http://doi.org/10.3341/jkos.2017.58.2.235
Abstract
- PURPOSE
We report a case of infraduction limitation improvement and orthotropia at primary position in a patient with traumatic isolated inferior rectus muscle rupture after immediate repair surgery of the ruptured muscle.
CASE SUMMARY
A 47-year-old man came to our emergency department complaining of right eyelid contusion and conjunctival laceration after trauma due to the metal part of a high pressure hose. Right hypertropia of 20 prism diopters was observed at primary gaze and right hypertropia of 30 prism diopters was observed at down gaze. The right eye showed a -4 infraduction limitation. We sutured the distal part of the ruptured inferior rectus muscle with surrounding tissue, including the Tenon's capsule and the part of the muscle stump, to its original insertion. Orthotropia at primary position and 8-prism-diopters of right hypertropia on down gaze was observed one day after surgery. At 40 days after surgery, the patient had orthotropia at primary position and 4-prism-diopter right hypertropia on down gaze. Infraduction limitation of the right eye improved to -1.
CONCLUSIONS
Immediate repair of complete traumatic isolated inferior rectus muscle rupture can correct the limitation of extraocular movement and achieve orthotropia at primary position.
MeSH Terms
Figure
-
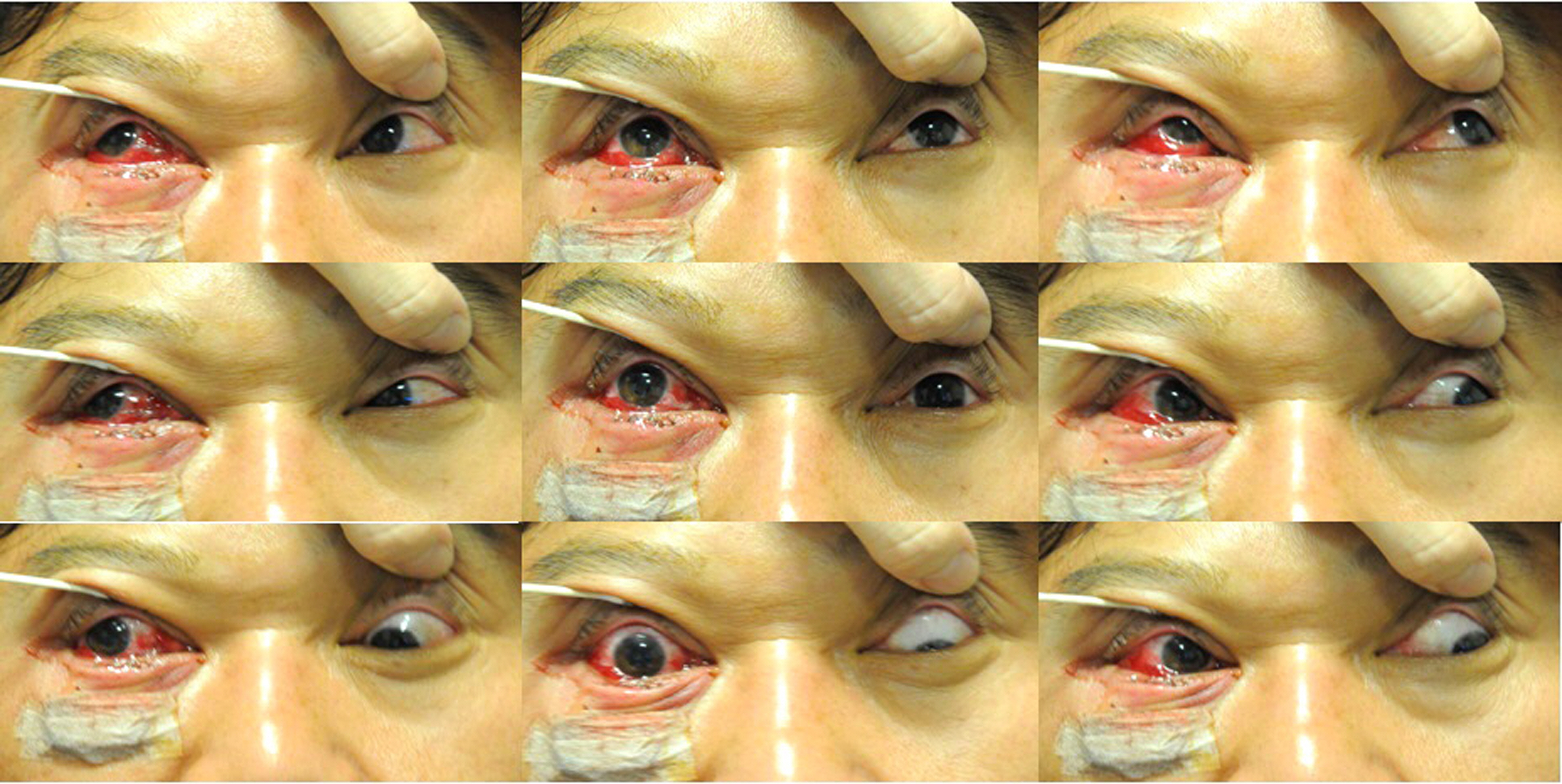
Figure 1. Preoperative clinical findings. Right hypertropia is noted at primary position and down gaze. Right eye reveals marked limitation of depression.
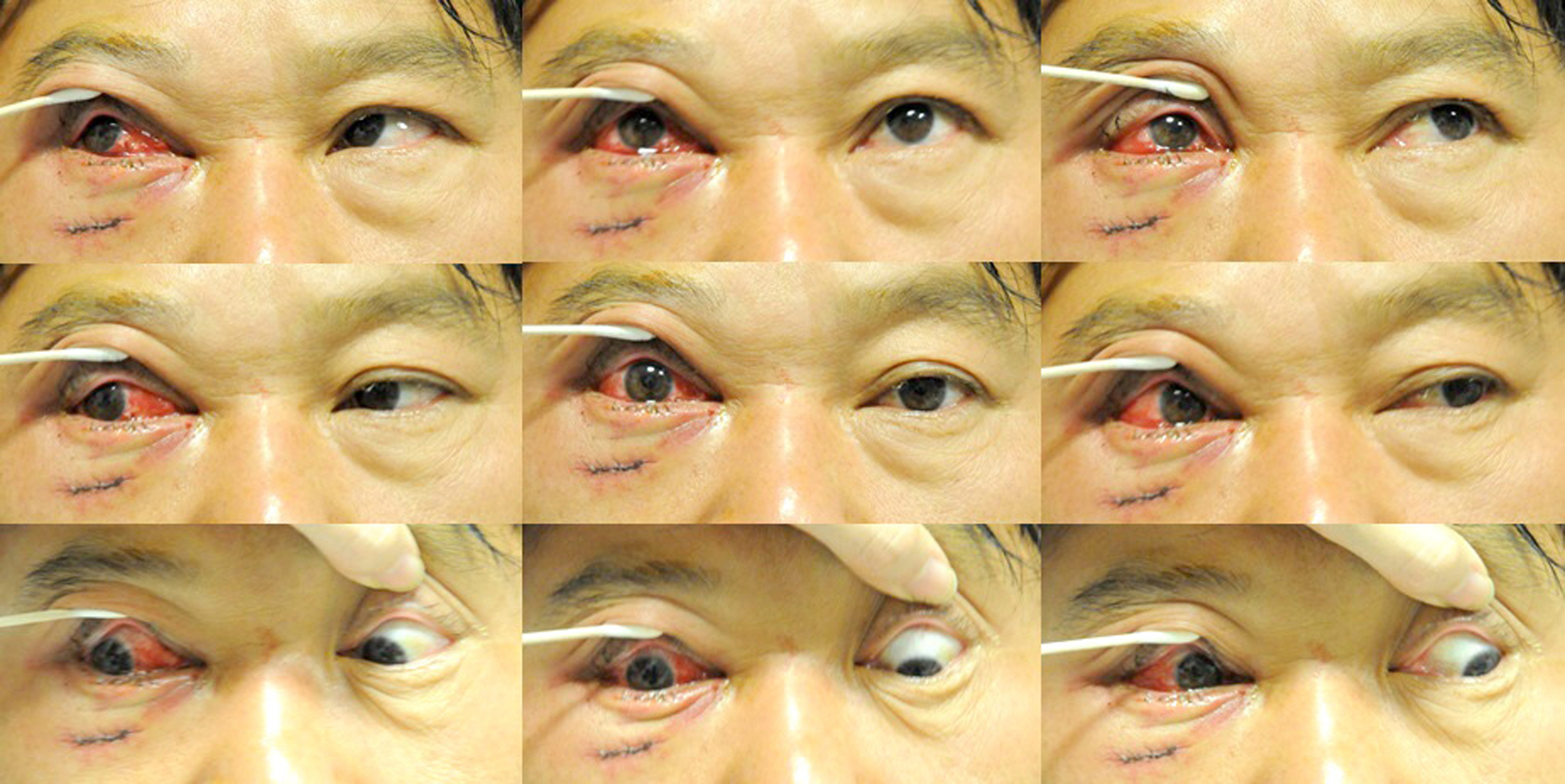
Figure 2. Postoperative clinical findings at the 1st day after surgery. Improvement of right hypertropia is noted at primary position.

Figure 3. Postoperative clinical findings at 40 days after surgery. Improvement of infraduction of the right eye and right hypertropia are shown.
Reference
-
References
1. Çağ atay HH, Ekinci M, Ulusal Ş. . Isolated rectus muscle rup-ture following trauma. Nepal J Ophthalmol. 2015; 7:182–5.2. Batra R, Gao A, Shun-Shin GA. The management of traumatic iso-lated inferior rectus rupture. Strabismus. 2012; 20:105–8.
Article3. Gupta M, Chadha V, Vallance J, Kearns P. Isolated inferior rectus rupture and inverse Knapp procedure: a rare condition with an un-common treatment. Asian J Ophthalmol. 2008; 10:180–1.4. Shin SY, Kim DS, Shin JC. A case of ocular torticollis associated with inferior rectus muscle transection. J Korean Ophthalmol Soc. 2000; 41:294–8.5. Cherfan CG, Traboulsi EI. Slipped, severed, torn and lost extra-ocular muscles. Can J Ophthalmol. 2011; 46:501–9.
Article6. Min BM, Jung SY. The effect of anterior transposition of the in-ferior oblique muscle with marginal myectomy in a case of lost in-ferior rectus muscle. J Korean Ophthalmol Soc. 1996; 37:1973–8.7. Richards R. Ocular motility disturbances following trauma. Adv Ophthalmic Plast Reconstr Surg. 1987; 7:133–47.8. Kushner BJ, Sprunger DT, Saunders RA. . Grand rounds #50: A case of a lost medial rectus muscle in an eye in which the inferior rectus muscle "pulled in two". Binocul Vis Strabismus Q. 1998; 13:116–23.9. Ling R, Quinn AG. Traumatic rupture of the medial rectus muscle. J AAPOS. 2001; 5:327–8.
Article10. Kashima T, Akiyama H, Kishi S. Longitudinal tear of the inferior rectus muscle in orbital floor fracture. Orbit. 2012; 31:171–3.
Article11. Sloan B, McNab AA. Inferior rectus rupture following blowout fracture. Aust N Z J Ophthalmol. 1998; 26:171–3.
Article12. Paysse EA, Saunders RA, Coats DK. Surgical management of stra-bismus after rupture of the inferior rectus muscle. J AAPOS. 2000; 4:164–7.
Article13. Helveston EM, Grossman RD. Extraocular muscle lacerations. Am J Ophthalmol. 1976; 81:754–60.
Article14. Tomasetti P, Metzler P, Jacobsen C. Isolated inferior rectus muscle rupture after blunt orbital trauma. J Surg Case Rep. 2013; 2013(pii):rjt076.
Article15. Cronin CM, Mittelman D, Folk ER, Moore D. Transection of the inferior rectus muscle. J Pediatr Ophthalmol Strabismus. 1986; 23:239–45.
Article16. Godeiro KD, Pinto AG. . Traumatic tear of the inferior rectus muscle treated with inferior oblique anterior transposition. Int Ophthalmol. 2005; 26:185–9.
Article17. Parks MM. Rosembaum A, editor. Slipped, disinserted or severed, and lost muscles. Clinical Strabismus Management. Philadelphia: WB Saunders;1999; 529–38.18. Hayreh SS, Scott WE. Fluorescein iris angiography. II. Disturbances in iris circulation following strabismus operation on the various recti. Arch Ophthalmol. 1978; 96:1390–400.19. Virdi PS, Hayreh SS. Anterior segment ischemia after recession of various recti. An experimental study. Ophthalmology. 1987; 94:1258–71.20. Metz HS. 20th annual Frank Costenbader Lecture-muscle trans-position surgery. J Pediatr Ophthalmol Strabismus. 1993; 30:346–53.
Article21. O'Toole L, Long V, Power W, O'Connor M.Traumatic rupture of the lateral rectus. Eye (Lond). 2004; 18:221–2.22. Huerva V, Mateo AJ, Espinet R. Isolated medial rectus muscle rup-ture after a traffic accident. Strabismus. 2008; 16:33–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Congenital Absence of the Inferior Rectus Muscle
- Resection and Transposition of the Inferior Oblique for Hypertropia due to the Inferior Rectus Loss
- The Effect of Anteriorization of The Inferior Oblique Muscle in +3 or +4 Inferior Oblique Overaction
- Isolated Inferior Rectus Palsy from Midbrain Infarction
- The Effect of Modified Anterior Transposition of the Inferior Oblique Muscle for Hypertropia in Superior Oblique Muscle Palsy with Inferior Oblique Muscle Overaction
