Immediate Postoperative Intraocular Pressure Adjustment Reduces Risk of Cystoid Macular Edema after Uncomplicated Micro Incision Coaxial Phacoemulsification Cataract Surgery
- Affiliations
-
- 1Department of Ophthalmology, Mason Eye Institute, University of Missouri School of Medicine, Columbia, MO, USA. jarstadj@health.missouri.edu
- 2Department of Ophthalmology, SUNY-Upstate Medical University, Syracuse, NY, USA.
- 3Cornea and External Disease Service, Evergreen Eye Center, Federal Way, WA, USA.
- 4Evergreen Eye Center, Federal Way, WA, USA.
- 5Retina Service, Evergreen Eye Center, Federal Way, WA, USA.
- KMID: 2368677
- DOI: http://doi.org/10.3341/kjo.2017.31.1.39
Abstract
- PURPOSE
To determine the accuracy of visual estimation of immediate postoperative intraocular pressure (IOP) following microincision cataract surgery (MICS) and the effect of immediate postoperative IOP adjustment on prevention of cystoid macular edema (CME). SETTING: Ambulatory surgical center.
METHODS
Prospective, randomized analysis of 170 eyes in 135 patients with MICS, performed in a Medicare approved outpatient ambulatory surgery center. Surgical parameters included a keratome incision of 1.5 mm to 2.8 mm, topical anesthetic, case completion IOP estimation by palpation and patient visualization of light, and IOP adjustment before exiting the operating theater. IOPs were classified into three groups: low (<16 mmHg), normal (16 to 21 mmHg), and elevated (>21 to 30 mmHg). IOP measurements were repeated 1 day after surgery. Optical coherence tomography (Stratus OCT, Zeiss) was measured at 2 weeks. An increase in foveal thickness greater than 15 µm was used to indicate CME. Statistical analysis was performed using one- and two-tailed Student's t-tests.
RESULTS
Mean minimal foveal thickness averaged 207.15 µm in the low pressure group, 205.14 µm in the normal IOP group, and 210.48 µm in the elevated IOP group 2 weeks following surgery. CME occurred in 14 of 170 eyes (8.2%) at 2 weeks (low IOP, 35.7%; normal IOP, 14.2%; elevated IOP, 50.0%). Change in IOP from the operating theater to 1 day after surgery was within +/−5 mmHg in 54 eyes (31.7%), elevated by 6 to 15 mmHg in 22 eyes (12.9%), and elevated more than 15 mmHg in four eyes (2.3%). IOP was reduced by 6 mmHg to 15 mmHg in 39 eyes (22.9%) and reduced by more than 15 mmHg in nine eyes (5.3%).
CONCLUSIONS
Immediate postoperative adjustment of IOP may prevent CME in MICS. Physicians can improve their ability to estimate postoperative IOP with experience in tonometry to verify immediate postoperative IOP. There are patient safety and economic benefits to immediate IOP adjustment in the operating theater. SYNOPSIS: Immediate postoperative IOP adjustment following cataract surgery before the patient leaves the operating theater may reduce the incidence of CME and provide patient safety and economic benefits.
MeSH Terms
Figure
-

Fig. 1 Case completion estimated intraocular pressure by surgeon. Immediate unadjusted postoperative intraocular pressure estimates varied by surgeon and were initially inconsistent. These estimates improved with surgeon experience over the course of the study.
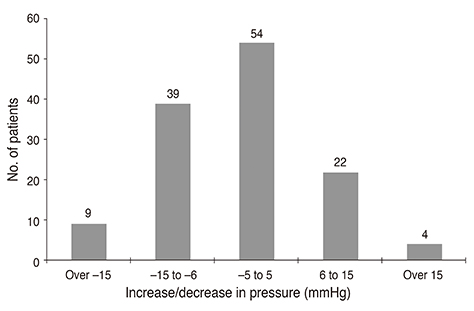
Fig. 2 Change in intraocular pressure (IOP) from case completion to 1-day postop. Change in adjusted IOP from the operating theater to 1-day postop. Note the distribution showing little change in IOP in the majority of cases from the IOP adjusted on the operating room table to the next day postop. postop = postoperative.

Fig. 3 Cystoid macular edema (CME) by intraocular pressure (IOP) group. Two week macular thickness in the adjusted IOP group. CME grouped by adjusted postoperative IOP. Note that IOP values greater than 22 mmHg were responsible for 50% of the cases of CME, while normally adjusted IOP had the lowest incidence. *Patients considered to have macular edema if surgical eye is 15 or more microns thicker than non-surgical eye.
Fig. 4 Rebound or “relative hypotony.” Illustration depicting rebound or relative hypotony from low intraocular pressure values. CME = cystoid macular edema.
Reference
-
1. Jurecka T, Batkova Z, Ventruba J. Macular edema after an uncomplicated cataract surgery. Cesk Slov Oftalmol. 2007; 63:262–273.2. El-Ashry M, Hegde V, James P, Pagliarini S. Analysis of macular thickness in British population using optical coherence tomography (OCT): an emphasis on interocular symmetry. Curr Eye Res. 2008; 33:693–699.3. Kecik D, Makowiec-Tabernacka M, Golebiewska J, et al. Macular thickness and volume after uncomplicated phacoemulsification surgery evaluated by optical coherence tomography: a one-year follow-up. Neuro Endocrinol Lett. 2009; 30:610–614.4. Burling-Phillips L. After cataract surgery: watching for cystoid macular edema [Internet]. San Francisco, CA: EyeNet;2007. cited 2017 Jan 13. Available from: http://www.aao.org/publications/eyenet/200701/retina.cfm.5. Yuksel N, Dogu B, Karabas VL, Caglar Y. Foveal thickness after phacoemulsification in patients with pseudoexfoliation syndrome, pseudoexfoliation glaucoma, or primary open-angle glaucoma. J Cataract Refract Surg. 2008; 34:1953–1957.6. Chao WJ, Liu SB, Dai RP, et al. Clinical analysis of intraocular pressure elevation following vitreoretinal surgery. Zhonghua Yi Xue Za Zhi. 2009; 89:318–320.7. Degenring RF, Vey S, Kamppeter B, et al. Effect of uncomplicated phacoemulsification on the central retina in diabetic and non-diabetic subjects. Graefes Arch Clin Exp Ophthalmol. 2007; 245:18–23.8. Biro Z, Balla Z, Kovacs B. Change of foveal and perifoveal thickness measured by OCT after phacoemulsification and IOL implantation. Eye (Lond). 2008; 22:8–12.9. Catier A, Tadayoni R, Paques M, et al. Characterization of macular edema from various etiologies by optical coherence tomography. Am J Ophthalmol. 2005; 140:200–206.10. Lobo CL, Faria PM, Soares MA, et al. Macular alterations after small-incision cataract surgery. J Cataract Refract Surg. 2004; 30:752–760.11. Cagini C, Fiore T, Iaccheri B, et al. Macular thickness measured by optical coherence tomography in a healthy population before and after uncomplicated cataract phacoemulsification surgery. Curr Eye Res. 2009; 34:1036–1041.12. Ching HY, Wong AC, Wong CC, et al. Cystoid macular oedema and changes in retinal thickness after phacoemulsification with optical coherence tomography. Eye (Lond). 2006; 20:297–303.13. Pareja-Esteban J, Moreno-Arrones JP, Drake-Rodriguez-Casanova P, et al. Morphological macular changes after cataract surgery: risk factors. Arch Soc Esp Oftalmol. 2009; 84:605–610.14. Belair ML, Kim SJ, Thorne JE, et al. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am J Ophthalmol. 2009; 148:128–135.e2.15. Rhee DJ, Deramo VA, Connolly BP, Blecher MH. Intraocular pressure trends after supranormal pressurization to aid closure of sutureless cataract wounds. J Cataract Refract Surg. 1999; 25:546–549.16. Levkovitch-Verbin H, Habot-Wilner Z, Burla N, et al. Intraocular pressure elevation within the first 24 hours after cataract surgery in patients with glaucoma or exfoliation syndrome. Ophthalmology. 2008; 115:104–108.17. Bui CM, Recchia FM, Recchia CC, Kammer JA. Optical coherence tomography findings in ocular decompression retinopathy. Ophthalmic Surg Lasers Imaging. 2006; 37:333–335.18. Vu MT, Shields MB. The early postoperative pressure course in glaucoma patients following cataract surgery. Ophthalmic Surg. 1988; 19:467–470.19. Hayreh SS. Anterior ischemic optic neuropathy. IV: occurrence after cataract extraction. Arch Ophthalmol. 1980; 98:1410–1416.20. Shingleton BJ, Rosenberg RB, Teixeira R, O'Donoghue MW. Evaluation of intraocular pressure in the immediate postoperative period after phacoemulsification. J Cataract Refract Surg. 2007; 33:1953–1957.21. Laurell CG, Lydahl E. Evaluation of aqueous outflow facility in patients with high intraocular pressure after cataract surgery. Ophthalmic Surg Lasers Imaging. 2006; 37:476–480.22. Tong JT, Miller KM. Intraocular pressure change after sutureless phacoemulsification and foldable posterior chamber lens implantation. J Cataract Refract Surg. 1998; 24:256–262.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Secondary Macular Hole Formation after Phacoemulsification in a Vitrectomized Eye
- Retinal Thickness After Cataract Surgery Measured by Optical Coherence Tomography
- Prophylactic Intracameral Vancomycin Irrigation and Cystoid Macular Edema
- Effect of Non-Steroidal Anti-Inflammatory Drugs on Cystoid Macular Edema in Diabetic Patients after Cataract Surgery
- Change in Central Macular Thickness after 2.2-mm Microincision Coaxial versus 2.75-mm Small Incision Cataract Surgery
