Cancer Res Treat.
2017 Jan;49(1):20-28. 10.4143/crt.2016.057.
Minimally Invasive Stereotactical Radio-ablation of Adrenal Metastases as an Alternative to Surgery
- Affiliations
-
- 1Department of Radiotherapy and Radiosurgery, Humanitas Cancer Center and Research Hospital, Milano, Italy. ciro.franzese@humanitas.it
- KMID: 2367499
- DOI: http://doi.org/10.4143/crt.2016.057
Abstract
- PURPOSE
The purpose of this study was to study the clinical outcome for patients with metastases of the adrenal gland treated with stereotactic body radiation therapy.
MATERIALS AND METHODS
Forty-six patients were studied retrospectively. The dose prescription was 40 Gy in four fractions. Dosimetric analysis was performed using the dose volume histograms while clinical outcome was assessed using actuarial analysis with determination of the overall survival (OS) and local control (LC) rates.
RESULTS
The planning objectives were met for all patients. With a median follow-up period of 7.6 months, at the last follow-up 42 patients (91.3%) were alive and four had died because of distant progression. The actuarial mean OS was 28.5±1.6 months, the median was not reached. One-year and 2-year OS were 87.6±6.1%. None of the risk factors was significant in univariate analysis. Actuarial mean LC was 14.6±1.8 months (95% confidence interval [CI], 11.0 to 18.2) and median LC was 14.5±2.0 months (95% CI, 10.5 to 18.5). One-year and 2-year LC were 65.5±11.9% and 40.7±15.8%, respectively. A mild profile of toxicity was observed in the cohort of patients. Forty patients (86.9%) showed no complication (grade 0); two patients reported asthenia, six patients (13.1%) reported either pain, nausea, or vomiting. Of these six patients, five patients (10.9%) were scored as grade 1 toxicity while one patient (2.2%) was scored as grade 2.
CONCLUSION
Stereotactic body radiation therapy treatment provided an adequate clinical response in the management of adrenal gland metastases.
MeSH Terms
Figure
-
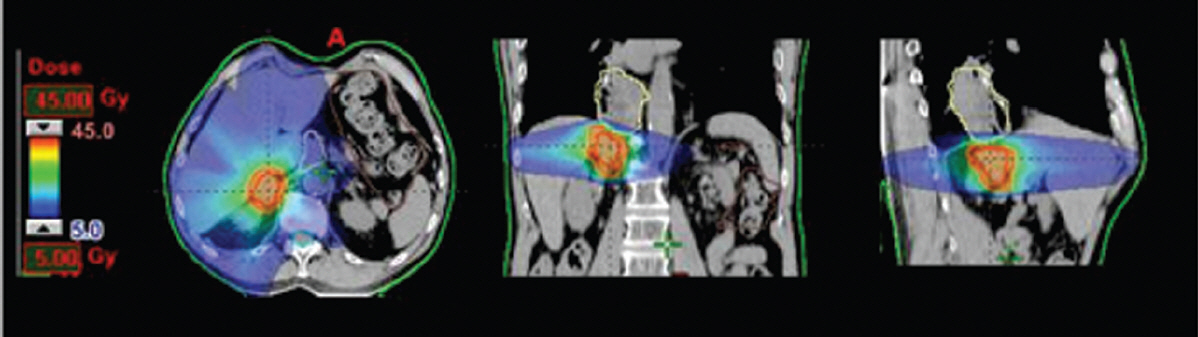
Fig. 1. Typical dose distribution (in colowash from 5 to 45 Gy) for axial, sagittal, and coronal views.

Fig. 2. Average dose volume histograms (blue line) and interpatient variability at 1 standard deviation (red lines) for target volumes and organs at risk.
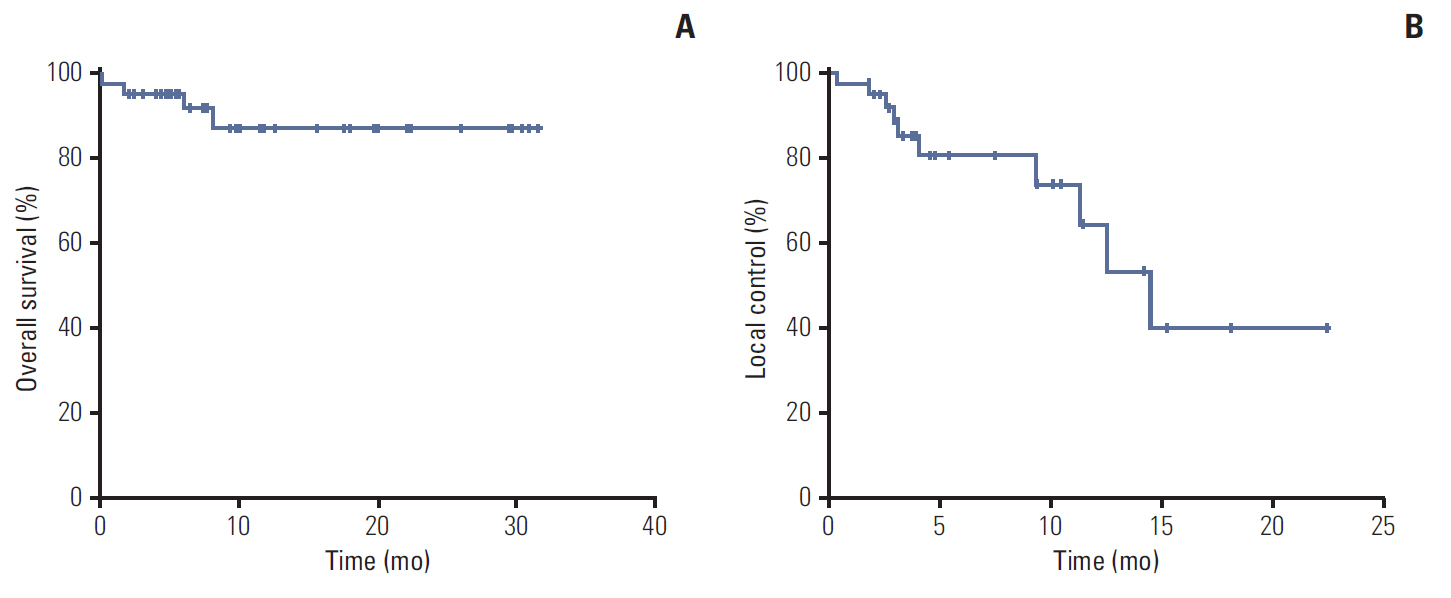
Fig. 3. Actuarial graphs for overall survival (A) and local control (B).
Reference
-
References
1. Lam KY, Lo CY. Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol (Oxf). 2002; 56:95–101.
Article2. Wansaicheong G, Goh J. Adrenal metastases [Internet]. New York: Medsacape;2016. [cited 2016 Mar 2]. Available from: http://www.emedicine.com/radio/TOPIC17.3. Oshiro Y, Takeda Y, Hirano S, Ito H, Aruga T. Role of radiotherapy for local control of asymptomatic adrenal metastasis from lung cancer. Am J Clin Oncol. 2011; 34:249–53.
Article4. Kumar R, Xiu Y, Yu JQ, Takalkar A, El-Haddad G, Potenta S, et al. 18F-FDG PET in evaluation of adrenal lesions in patients with lung cancer. J Nucl Med. 2004; 45:2058–62.5. Hellman S. Karnofsky Memorial Lecture: natural history of small breast cancers. J Clin Oncol. 1994; 12:2229–34.
Article6. Luketich JD, Burt ME. Does resection of adrenal metastases from non-small cell lung cancer improve survival? Ann Thorac Surg. 1996; 62:1614–6.
Article7. Mittendorf EA, Lim SJ, Schacherer CW, Lucci A, Cormier JN, Mansfield PF, et al. Melanoma adrenal metastasis: natural history and surgical management. Am J Surg. 2008; 195:363–8.
Article8. Muth A, Persson F, Jansson S, Johanson V, Ahlman H, Wangberg B. Prognostic factors for survival after surgery for adrenal metastasis. Eur J Surg Oncol. 2010; 36:699–704.
Article9. Kim SH, Brennan MF, Russo P, Burt ME, Coit DG. The role of surgery in the treatment of clinically isolated adrenal metastasis. Cancer. 1998; 82:389–94.
Article10. Uberoi J, Munver R. Surgical management of metastases to the adrenal gland: open, laparoscopic, and ablative approaches. Curr Urol Rep. 2009; 10:67–72.
Article11. Tanvetyanon T, Robinson LA, Schell MJ, Strong VE, Kapoor R, Coit DG, et al. Outcomes of adrenalectomy for isolated synchronous versus metachronous adrenal metastases in non-small-cell lung cancer: a systematic review and pooled analysis. J Clin Oncol. 2008; 26:1142–7.
Article12. Wood BJ, Abraham J, Hvizda JL, Alexander HR, Fojo T. Radiofrequency ablation of adrenal tumors and adrenocortical carcinoma metastases. Cancer. 2003; 97:554–60.
Article13. Hsieh MH, Lin ZY, Huang CJ, Shih MC, Chuang WL. Management of bilateral adrenal metastases from hepatocellular carcinoma: a case report. Kaohsiung J Med Sci. 2005; 21:371–6.
Article14. Duh QY. Resecting isolated adrenal metastasis: why and how? Ann Surg Oncol. 2003; 10:1138–9.
Article15. Soffen EM, Solin LJ, Rubenstein JH, Hanks GE. Palliative radiotherapy for symptomatic adrenal metastases. Cancer. 1990; 65:1318–20.
Article16. Short S, Chaturvedi A, Leslie MD. Palliation of symptomatic adrenal gland metastases by radiotherapy. Clin Oncol (R Coll Radiol). 1996; 8:387–9.
Article17. Alongi F, Arcangeli S, Filippi AR, Ricardi U, Scorsetti M. Review and uses of stereotactic body radiation therapy for oligometastases. Oncologist. 2012; 17:1100–7.
Article18. Scorsetti M, Mancosu P, Navarria P, Tozzi A, Castiglioni S, Clerici E, et al. Stereotactic body radiation therapy (SBRT) for adrenal metastases: a feasibility study of advanced techniques with modulated photons and protons. Strahlenther Onkol. 2011; 187:238–44.19. Gunjur A, Duong C, Ball D, Siva S. Surgical and ablative therapies for the management of adrenal 'oligometastases': a systematic review. Cancer Treat Rev. 2014; 40:838–46.20. Casamassima F, Livi L, Masciullo S, Menichelli C, Masi L, Meattini I, et al. Stereotactic radiotherapy for adrenal gland metastases: university of Florence experience. Int J Radiat Oncol Biol Phys. 2012; 82:919–23.
Article21. Chawla S, Chen Y, Katz AW, Muhs AG, Philip A, Okunieff P, et al. Stereotactic body radiotherapy for treatment of adrenal metastases. Int J Radiat Oncol Biol Phys. 2009; 75:71–5.
Article22. Katoh N, Onimaru R, Sakuhara Y, Abo D, Shimizu S, Taguchi H, et al. Real-time tumor-tracking radiotherapy for adrenal tumors. Radiother Oncol. 2008; 87:418–24.
Article23. Torok J, Wegner RE, Burton SA, Heron DE. Stereotactic body radiation therapy for adrenal metastases: a retrospective review of a noninvasive therapeutic strategy. Future Oncol. 2011; 7:145–51.
Article24. Holy R, Piroth M, Pinkawa M, Eble MJ. Stereotactic body radiation therapy (SBRT) for treatment of adrenal gland metastases from non-small cell lung cancer. Strahlenther Onkol. 2011; 187:245–51.
Article25. Ahmed KA, Barney BM, Macdonald OK, Miller RC, Garces YI, Laack NN, et al. Stereotactic body radiotherapy in the treatment of adrenal metastases. Am J Clin Oncol. 2013; 36:509–13.
Article26. Romero Arenas MA, Sui D, Grubbs EG, Lee JE, Perrier ND. Adrenal metastectomy is safe in selected patients. World J Surg. 2014; 38:1336–42.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic assisted adrenalectomy: Is it ready for prime time?
- Percutaneous Adrenal Radiofrequency Ablation: A Short Review for Endocrinologists
- Asian Conference on Tumor Ablation Guidelines for Adrenal Tumor Ablation
- Minimally Invasive Surgery in Endocrine Surgical Diseases
- A New Beginning for the Journal of Minimally Invasive Surgery for the International Recognition and Contribution of Scientific Development of Minimally Invasive Surgery
