Descent of mesonephric duct to the final position of the vas deferens in human embryo and fetus
- Affiliations
-
- 1Department of Anatomy, Histology and Embryology, Yanbian University Medical College, Yanji, China. zwjin@ybu.edu.cn
- 2Department of Anatomy, Akita University School of Medicine, Akita, Japan.
- 3Department of Urology, Kobe University School of Medicine, Kobe, Japan.
- 4Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan.
- 5Department of Anatomy and Human Embryology, Institute of Embryology, Faculty of Medicine, Complutense University, Madrid, Spain.
- KMID: 2365552
- DOI: http://doi.org/10.5115/acb.2016.49.4.231
Abstract
- Because the ureter arises from the mesonephric or Wolffian duct (WD), the WD opening should migrate inferiorly along the urogenital sinus or future urethra. However, this process of descent has not been evaluated morphometrically in previous studies and we know little about intermediate morphologies for the descent. In the present work, serial sagittal sections of 15 specimens at gestational age 6-12 weeks and serial horizontal sections of 20 specimens at 6-10 weeks were analyzed. Monitoring of horizontal sections showed that, until 9 weeks, a heart-, lozenge- or oval-shape of the initial urogenital sinus remained in the bladder and urethra. Thus, the future bladder and urethra could not be distinguished by the transverse section or plane. The maximum width of the urogenital sinus or bladder at 6-10 weeks was 0.8 mm, although its supero-inferior length reached 5 mm at 10 weeks. During earlier stages, however, the medial shift of the WD was rather evident. Depending on the extent of upward growth of the bladder smooth muscle, the descent of the vas deferens became evident at 10-12 weeks. Development of the urethral rhabdosphincter likely resulted in the differentiation of urogenital sinus into the urethra and bladder before formation of the bladder neck with 3-layered smooth muscles. Development of the prostate followed these morphological changes, later accelerating the further descent of the WD opening. Because of their close topographical relationships, slight anomalies or accidents of the umbilical cord at 10-12 weeks may have a significant effect on normal anatomy.
MeSH Terms
Figure
-

Fig. 1 Sagittal sections of two embryos before differentiation of urogenital sinus into the bladder and urethra. (A, B) A specimen of crown-rump length (CRL) 24 mm (7 weeks). (C–E) A specimen of CRL 35 mm (8 weeks). Hematoxylin and eosin staining. The left-hand side of each panel corresponds to the anterior side of the pelvis. Panel (A) (panel C) is the most medial side of panels (A) and (B) (panels C–E). Intervals between panels are 0.3 mm (A–B), 0.4 mm (C–D), and 0.2 mm (D–E), respectively. All panels were prepared at the same magnification. Scale bar in panel B=1 mm. (A, B) The Wolffian duct (WD) opening (arrow) is located less than 0.1 mm inferior and 0.3 mm medial side of the ureteral opening (arrowhead; UR). (D) The WD opening (arrow) is located 0.5 mm inferior and less than 0.1 mm medial side of the ureteral opening (arrowhead). (C) Smooth muscles start differentiation in the future bladder wall (stars), but the epithelium appears to be a common type of the urogenital sinus (URS). MD, Műllerian duct or paramesonephric duct; P, pubis; PC, peritoneal cavity; R, rectum; SMA, mesentery containing the superior mesenteric artery; ST, stomach; UA, umbilical artery; WD, Wolffian duct or mesonephric duct.
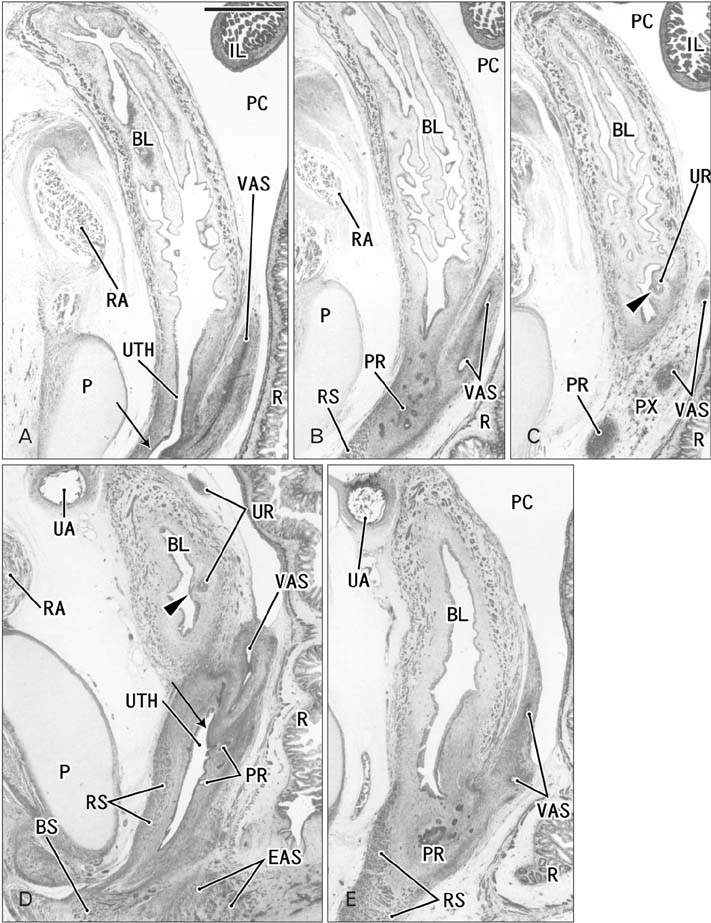
Fig. 2 Sagittal sections of two fetuses after differentiation of urogenital sinus into the bladder and urethra. (A–C) A specimen of crown-rump length (CRL) 56 mm (10 weeks). (D, E) A specimen of CRL 65 mm (12 weeks). Hematoxylin and eosin staining. The left-hand side of each panel corresponds to the anterior side of the pelvis. Panel (A) (panel D) is the most medial side of panels (A–C) (panels D and E). Intervals between panels are 1.1 mm (A–B), 1.5 mm (B–C), and 0.5 mm (D–E), respectively. All panels were prepared at the same magnification. Scale bar in panel A=1 mm. (A–C) The Wolffian duct (WD) opening (arrow) is located 2.2 mm inferior and 2.6 mm medial side of the ureteral opening (arrowhead; UR). (D) The WD opening (arrow) is located 1.9 mm inferior and less than 0.1 mm medial side of the ureteral opening (arrowhead). Smooth muscles are seen in the bladder wall (BL in all panels; dark red color), while the urethra (UTH) accompanies the rhabdophincter (RS in panels B, D, and E). The prostate (PR) starts developing as sprouts from the urethra in both specimens. EAS, external anal sphincter; IL, ileum of the intestine; P, pubis; PC, peritoneal cavity; PX, pelvic autonomic nerve plexus; R, rectum; RA, rectus abdominis muscle; UA, umbilical artery; VAS, vas deferens.
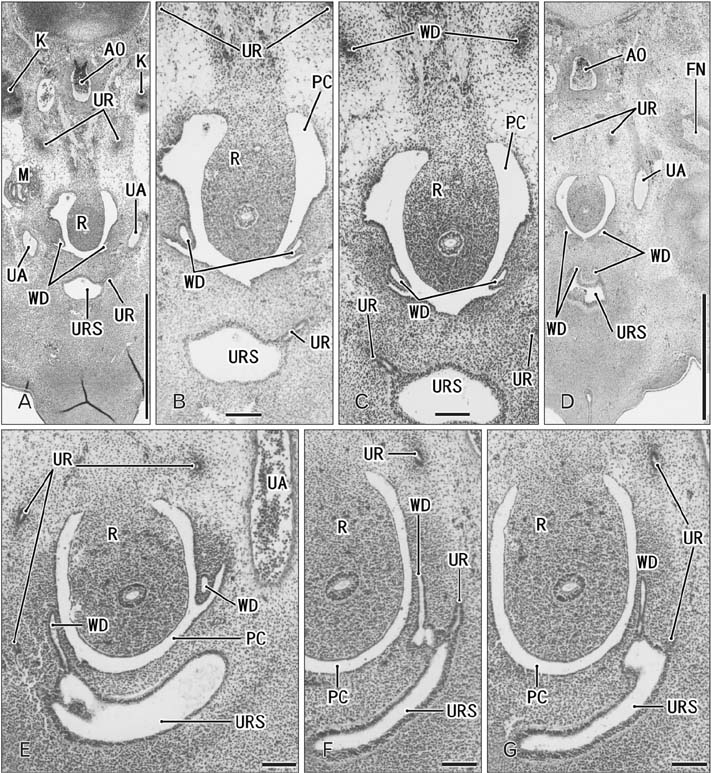
Fig. 3 Horizontal sections of two embryos at 6 weeks before differentiation of urogenital sinus into the bladder and urethra. (A–D) A specimen of crownrump length (CRL) 15 mm. (E–G) A specimen of CRL 17 mm. Hematoxylin and eosin staining. The upper side of each panel corresponds to the posterior side of the pelvis. Panel A (panel E) is the most superior side of panels (A–D) (panels E–G). Panel (B) is a higher magnification view of the central part of panel (A), panel (C) displays a plane 0.1 mm inferior side of panel (A) and 0.2 mm superior side of panel (D). Intervals between panels are 0.2 mm (E–F) and 0.1 mm (F–G), respectively. Scale bars=1 mm in panels A and D, 0.1 mm in panels B, C, and E–G. (A–D) The Wolffian duct (WD) opening is located 0.2–0.3 mm inferior and 0.1–0.2 mm medial side of the ureteral opening (UR). (F) The WD opening is located in the same supero-inferior level as and in 0.1 mm medial side of the ureteral opening. Because of the inferiorly hanging course, the unilateral ureter is cut at multiple sites in all panels. AO, aorta; FN, femoral nerve; K, definite kidney (metanephros); M, mesonephros; PC, peritoneal cavity; R, rectum; UA, umbilical artery; URS, urogenital sinus.
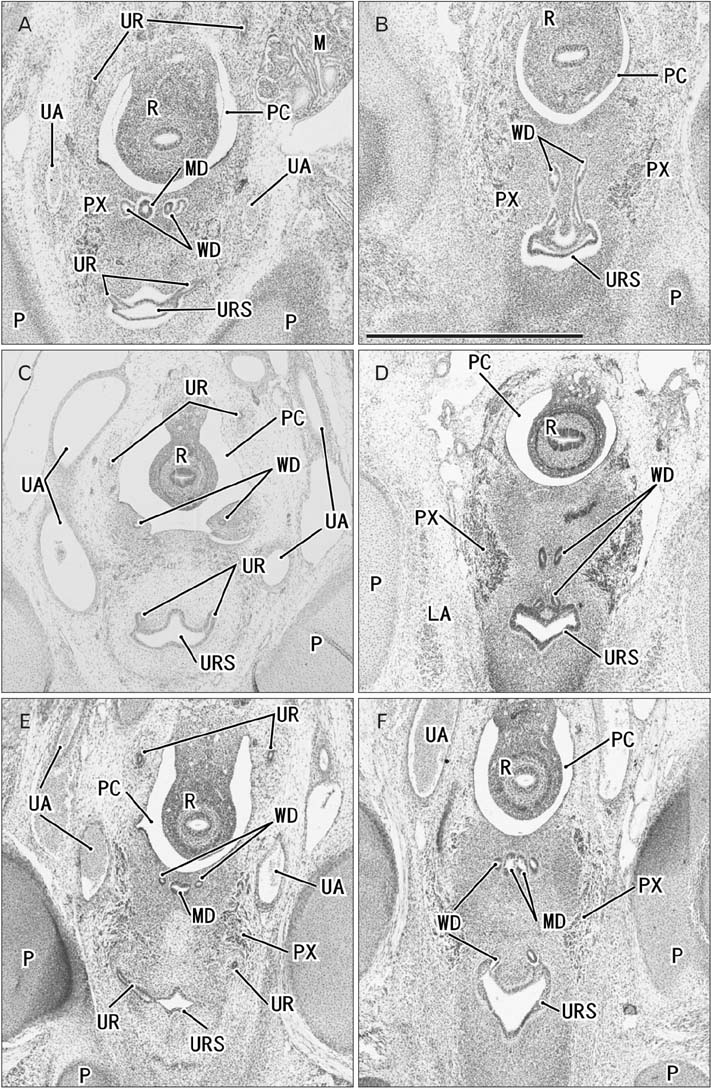
Fig. 4 Horizontal sections of three embryos at 7 weeks before differentiation of urogenital sinus into the bladder and urethra. (A, B) A specimen of crown-rump length (CRL) 21 mm. (C, D) A specimen of CRL 22 mm. (E, F) A specimen of CRL 26.5 mm. Hematoxylin and eosin staining. The upper side of each panel corresponds to the posterior side of the pelvis. Panels (A), (C), and (E) display the plane 0.2 mm, 0.3 mm, or 0.4 mm superior to panels (B), (D), or (F), respectively. All panels were prepared at the same magnification. Scale bar in panel B=1 mm. (A, B) The Wolffian duct (WD) opening is located 0.2 mm inferior and less than 0.1 mm medial side of the UR. (C, D) The WD opening is located 0.3 mm inferior and 0.1 mm medial side of the ureteral opening (UR). (E, F) The WD opening is located 0.3–0.4 mm inferior and less than 0.1 mm medial side of the UR. Because of the inferiorly hanging course, the unilateral ureter is cut at multiple sites in panels (A), (C), and (E). LA, levator ani muscle; M, mesonephros; MD, Műllerian duct or paramesonephric duct; P, pubis; PC, peritoneal cavity; PX, pelvic autonomic nerve plexus; R, rectum; UA, umbilical artery; URS, urogenital sinus.
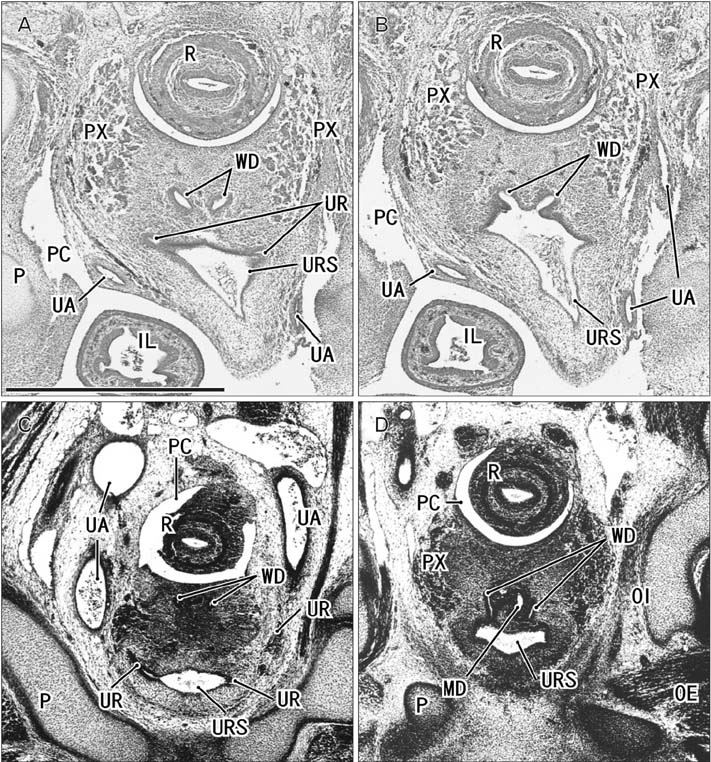
Fig. 5 Horizontal sections of two embryos at 7 weeks before differentiation of urogenital sinus into the bladder and urethra. (A, B) A specimen of crownrump length (CRL) 26 mm. (C, D) Another specimen of CRL 26 mm. Orange-G staining (A, B) and silver staining (C, D). The upper side of each panel corresponds to the posterior side of the pelvis. (A, B) The urogenital sinus (URS) is dilated and protrudes anteriorly due to unknown reason. Panels (A) and (C) display the plane 0.1 mm superior to panels (B) and (D), respectively. In both specimens, the Wolffian duct (WD) opening is located 0.1 mm inferior and 0.1 mm medial side of the ureteral opening (UR). All panels were prepared at the same magnification. Scale bar in panel A=1 mm. IL, ileum of the intestine; K, definite kidney (metanephros); MD, Műllerian duct or paramesonephric duct; OE, obturator externus muscle; OI, obturator internus muscle; P, pubis; PC, peritoneal cavity; PR, prostate; PX, pelvic autonomic nerve plexus; R, rectum; UA, umbilical artery.
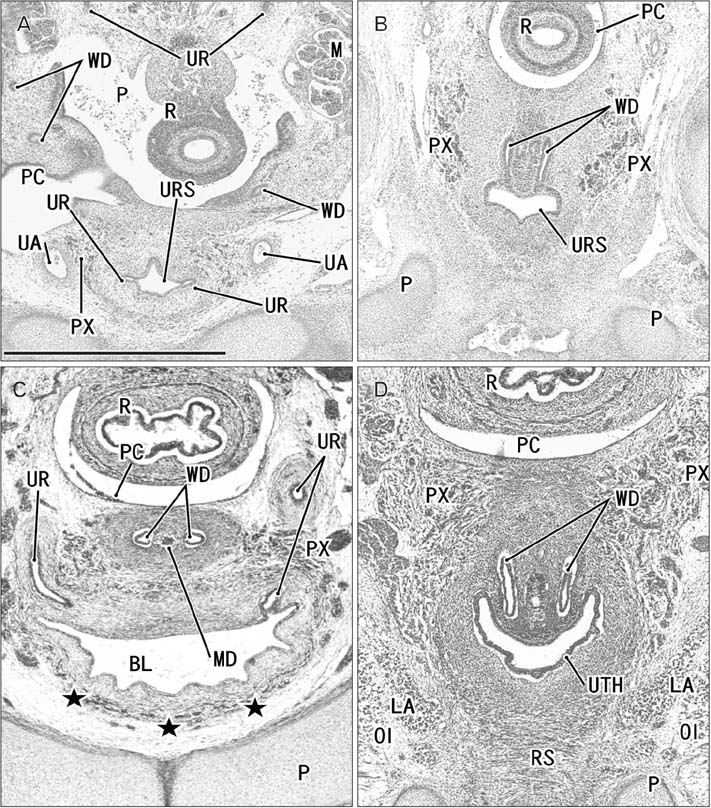
Fig. 6 Horizontal sections of two embryos at 8 weeks after differentiation of urogenital sinus into the bladder and urethra. (A, B) A specimen of crown-rump length (CRL) 29 mm. (C, D) A specimen of CRL 28 mm. Hematoxylin and eosin staining (A–C) and Orange-G staining (D). The upper side of each panel corresponds to the posterior side of the pelvis. Panels (A) and (C) display the plane 0.3 mm superior to panels (B) and (D), respectively. (C, D) In spite of the similar epithelium between sites, smooth muscles (stars) are evident in the bladder anterior wall (BL), while rhabdosphincter muscles (RS) develop along the urethra (UTH). In both specimens, the Wolffian duct (WD) opening is located 0.3 mm inferior and less than 0.1 mm medial side of the ureteral opening (UR). All panels were prepared at the same magnification. Scale bar in panel A=1 mm. BL, bladder; LA, levator ani muscle; M, mesonephros; MD, Műllerian duct or paramesonephric duct; OI, obturator internus mus c l e ; P, pubi s ; PC, peritoneal cavity; PX, pelvic autonomic nerve plexus; R, rectum; UA, umbilical artery; URS, urogenital sinus.
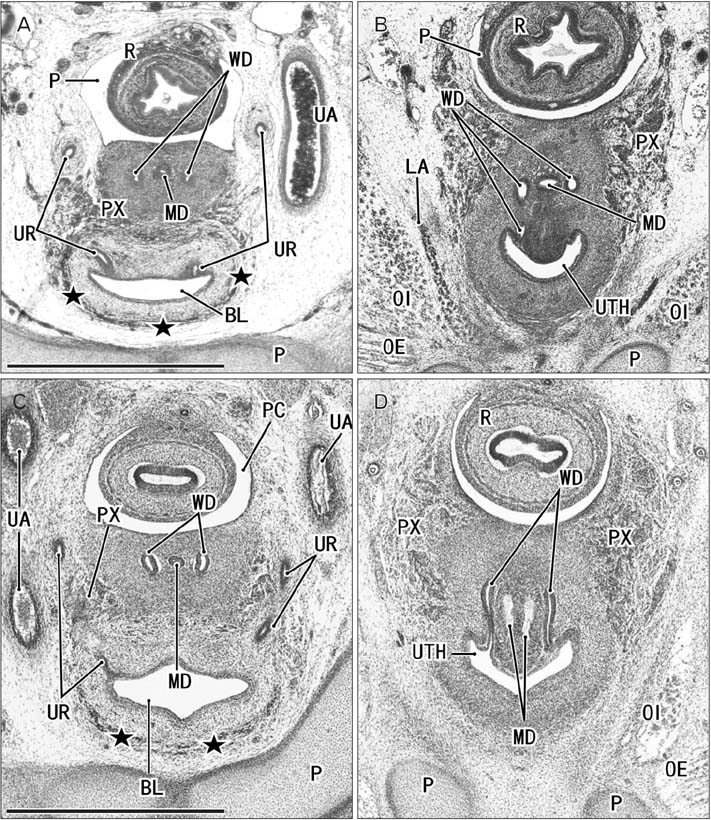
Fig. 7 Horizontal sections of two fetuses at 9 weeks after differentiation of urogenital sinus into the bladder and urethra. (A, B) A specimen of crownrump length (CRL) 39 mm. (C, D) A specimen of CRL 35 mm. Hematoxylin and eosin staining. The upper side of each panel corresponds to the posterior side of the pelvis. Panels A (or panel C) displays the plane 0.6 mm (or 0.8 mm) superior to panel B (or D), respectively. In both specimens, smooth muscles (stars) are evident in the bladder anterior wall (BL). In panels A and B (or C and D), the Wolffian duct (WD) opening is located 0.6 mm (or 0.8 mm) inferior and 0.1 mm medial side of the ureteral opening (UR). All panels were prepared at the same magnification. Scale bar in panel A=1 mm. LA, levator ani muscle; MD, Műllerian duct or paramesonephric duct; OE, obturator externus muscle; OI, obturator internus muscle; P, pubis; PC, peritoneal cavity; PX, pelvic autonomic nerve plexus; R, rectum; UA, umbilical artery; UTH, urethra.
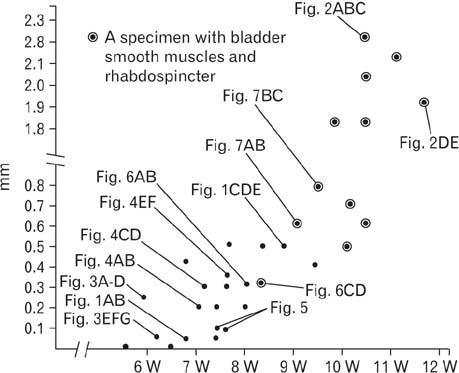
Fig. 8 Correlation between a gestational age and a topographical relation between the ureter and the Wolffian duct or vas deferens. One dot (a simple dot or a dot with circle) corresponds to one specimen. Thirty-two of the 35 specimens observed were evaluated because, in 3 specimens, a complete set of serial sections were not available. The dot with circle indicates a fact that, in the specimen, bladder smooth muscles as well as urethral rhabdosphincter muscles were evident. Depending on drastic development and growth of these muscles, the descent of the vas deferens rapidly occurs at 10–11 weeks. This change are not correlate with individual variations (Figs. 3,4,5,6,7) in the transverse shape and size of the urogenital sinus, bladder and urethra.
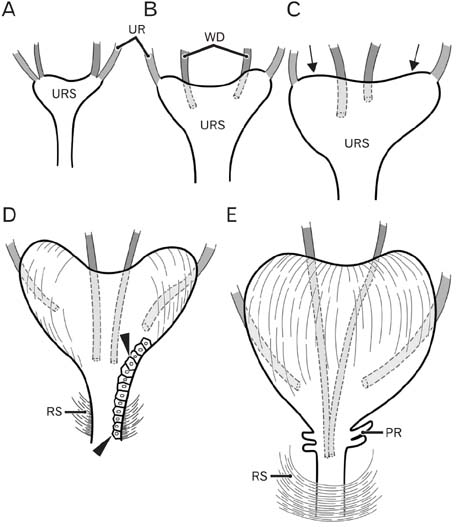
Fig. 9 Schematic representations of the descent of the Wolffian duct (WD) or vas deferens. Anterior view. At 6 weeks (A), the WD (red) opens to the urogenital sinus at a site adjacent to the ureteral orifice (UR; green). At 7–8 weeks (B, C), rather than descent, there are individual variations in the WD position along the mediolateral axis as well as in left/right difference in morphology of the urogenital sinus (URS). The future bladder and urethra are not discriminated in the sinus. At 8–9 weeks, the bilateral upper angles (arrows) of the URS start upward growth toward the umbilicus. At 9 weeks (D), depending on development of smooth muscles in the bladder as well as rhapdosphincter muscles of the urethra (RS), the descent of the vas deferens becomes evident. However, the epithelium is still same (arrowheads) between the future bladder and urethra. At 10–11 weeks (E), a drastic upward growth of bladder smooth muscles as well as a developing prostate (PR) accelerates the descent of the vas.
Reference
-
1. Hamilton WJ, Mossman HW. Human embryology. 4th ed. London: Williams & Wilkins;1978. p. 321–322.2. O'Rhahilly R, Műller F. Human embryology and teratology. 2nd ed. New York: Wiley-Liss;1996. p. 194–201.3. Moore KL, Persaud TV. The developing human: clinically oriented embryology. 6th ed. Philadelphia: Saunders;1998. p. 244–260.4. Naito M, Hinata N, Rodriguez-Vazquez JF, Murakami G, Aizawa S, Fujisawa M. Absorption of the Wolffian duct and duplicated ureter by the urogenital sinus: morphological study using human fetuses and embryos. BJU Int. 2015; 116:135–141.5. Masumoto H, Rodríguez-Vázquez JF, Verdugo-López S, Murakami G, Matsubara A. Fetal topographical anatomy of the female urethra and descending vagina: a histological study of the early human fetal urethra. Ann Anat. 2011; 193:500–508.6. Mendelsohn C. Using mouse models to understand normal and abnormal urogenital tract development. Organogenesis. 2009; 5:306–314.7. Tanaka ST, Ishii K, Demarco RT, Pope JC 4th, Brock JW 3rd, Hayward SW. Endodermal origin of bladder trigone inferred from mesenchymal-epithelial interaction. J Urol. 2010; 183:386–391.8. Evatt EJ. A contribution to the development of the prostate gland in the human female, and a study of the homologies of the urethra and vagina of the sexes. J Anat Physiol. 1911; 45(Pt 2):122–130.9. Parrott TS, Gray SW, Skandalakis JE. Bladder and urethra. In : Skandalakis JE, Gray SW, editors. Embryology for Surgeons. 2nd ed. Baltimore: Williams & Wilkins;1994. p. 671–717.10. Suson KD, Novak TE, Gupta AD, Benson J, Sponseller P, Gearhart JP. Neuro-orthopedic manifestations of the omphalocele exstrophy imperforate anus spinal defects complex. J Urol. 2010; 184:4 Suppl. 1651–1655.11. Kim JH, Hwang SE, Rodríguez-Vázquez JF, Murakami G, Cho BH. Liver agenesis with omphalocele: a report of two human embryos using serial histological sections. Pediatr Dev Pathol. 2014; 17:431–440.12. Fuchs F, Picone O, Levaillant JM, Mabille M, Mas AE, Frydman R, Senat MV. Prenatal diagnosis of a patent urachus cyst with the use of 2D, 3D, 4D ultrasound and fetal magnetic resonance imaging. Fetal Diagn Ther. 2008; 24:444–447.13. Bischoff A, Calvo-Garcia MA, Baregamian N, Levitt MA, Lim FY, Hall J, Peña A. Prenatal counseling for cloaca and cloacal exstrophy-challenges faced by pediatric surgeons. Pediatr Surg Int. 2012; 28:781–788.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Duplicated Vas Deferens Found Incidentally during Varicocelectomy
- A Case Report of Bilateral Absence of Vas Deferens
- Effect of antiandrogens upon the morphological development of gubernaculum and the testicular descent in rats
- Vas anomaly associated with ipsilateral renal hypoplasia
- Pharmacological Effects on Vas Deferens
