Korean J Pain.
2017 Jan;30(1):59-61. 10.3344/kjp.2017.30.1.59.
Fluoroscopy-guided intra-articular steroid injection for sternoclavicular joint arthritis secondary to limited cutaneous systemic sclerosis: a case report
- Affiliations
-
- 1Department of Algology, Kayseri Training and Research Hospital, Kayseri, Turkey. savas-44@hotmail.com
- 2Division of Algology, Department of Physical Medicine and Rehabilitation, Erciyes University, School of Medicine, Kayseri, Turkey.
- 3Department of Physical Medicine and Rehabilitation, Kayseri Training and Research Hospital, Kayseri, Turkey.
- 4Division of Rheumatology, Department of Physical Medicine and Rehabilitation, Erciyes University, School of Medicine, Kayseri, Turkey.
- KMID: 2365342
- DOI: http://doi.org/10.3344/kjp.2017.30.1.59
Abstract
- We report a case of fluoroscopy-guided intraarticular steroid injection for sternoclavicular joint (SCJ) arthritis caused by limited cutaneous systemic sclerosis (SSc). A 50-year-old woman diagnosed with limited cutaneous SSc presented with swelling and pain in the right SCJ. MRI revealed signs of inflammation consistent with right-sided sternoclavicular joint arthritis. After the failure of oral medications, we performed fluoroscopy-guided injection in this region. She reported complete resolution of her symptoms at 4 and 12-week follow-ups. This outcome suggests that a fluoroscopy-guided SCJ injection might be a safe and successful treatment option for sternoclavicular joint arthritis.
Keyword
MeSH Terms
Figure
-
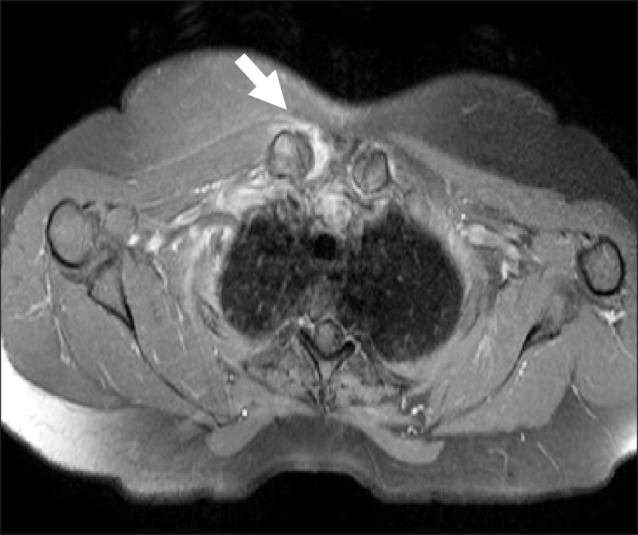
Fig. 1 T2-weighted axial MRI image showing fluid collection in the sternoclavicular joint (arrow).

Fig. 2 Contrast spread inside SCJ sternoclavicular joint.
Reference
-
1. Merlino G, Germano S, Carlucci S. Surgical management of digital calcinosis in CREST syndrome. Aesthetic Plast Surg. 2013; 37:1214–1219. PMID: 24142114.
Article2. Velayos EE, Masi AT, Stevens MB, Shulman LE. The 'CREST' syndrome. Comparison with systemic sclerosis (scleroderma). Arch Intern Med. 1979; 139:1240–1244. PMID: 508020.
Article3. Elhai M, Meunier M, Matucci-Cerinic M, Maurer B, Riemekasten G, Leturcq T, et al. Outcomes of patients with systemic sclerosis-associated polyarthritis and myopathy treated with tocilizumab or abatacept: a EUSTAR observational study. Ann Rheum Dis. 2013; 72:1217–1220. PMID: 23253926.
Article4. Joines MM, Motamedi K, Seeger LL, DiFiori JP. Musculoskeletal interventional ultrasound. Semin Musculoskelet Radiol. 2007; 11:192–198. PMID: 18095250.
Article5. Hassett G, Barnsley L. Pain referral from the sternoclavicular joint: a study in normal volunteers. Rheumatology (Oxford). 2001; 40:859–862. PMID: 11511753.
Article6. Galla R, Basava V, Conermann T, Kabazie AJ. Sternoclavicular steroid injection for treatment of pain in a patient with Osteitis condensans of the clavicle. Pain Physician. 2009; 12:987–990. PMID: 19935983.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Intra-articular Injection of Steroid on Lysozyme Activity in Patient with Rheumatoid Arthritis
- Fluoroscopy-Guided Intra-Articular Facet Joint Steroid Injection for the Management of Low Back Pain: Therapeutic Effectiveness and Arthrographic Pattern
- Efficacy of FluoroscopyGuided Lumbar Facet Joint Synovial Cyst Rupture with Intra-Articular Steroid Injection after Laminectomy
- Ultrasound-guided Intra-Articular Injections
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
