Chondroblastoma with Secondary Aneurysmal Bone Cyst in the Sphenoid Sinus: A Case Report
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea. midosyu@eulji.ac.kr
- 2Department of Neurosurgery, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- 3Department of Pathology, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 2365053
- DOI: http://doi.org/10.3348/jksr.2017.76.1.61
Abstract
- Chondroblastomas are rare benign cartilaginous neoplasms found in young patients. These tumors typically arise in the epiphysis or apophysis of a long bone. Chondroblastomas arising in the skull and facial bones are extremely rare. We describe a rare case of a patient presenting with chondroblastoma with secondary aneurysmal bone cyst in the sphenoid sinus that mimicked invasive sinusitis or malignant bone tumor.
MeSH Terms
Figure
-
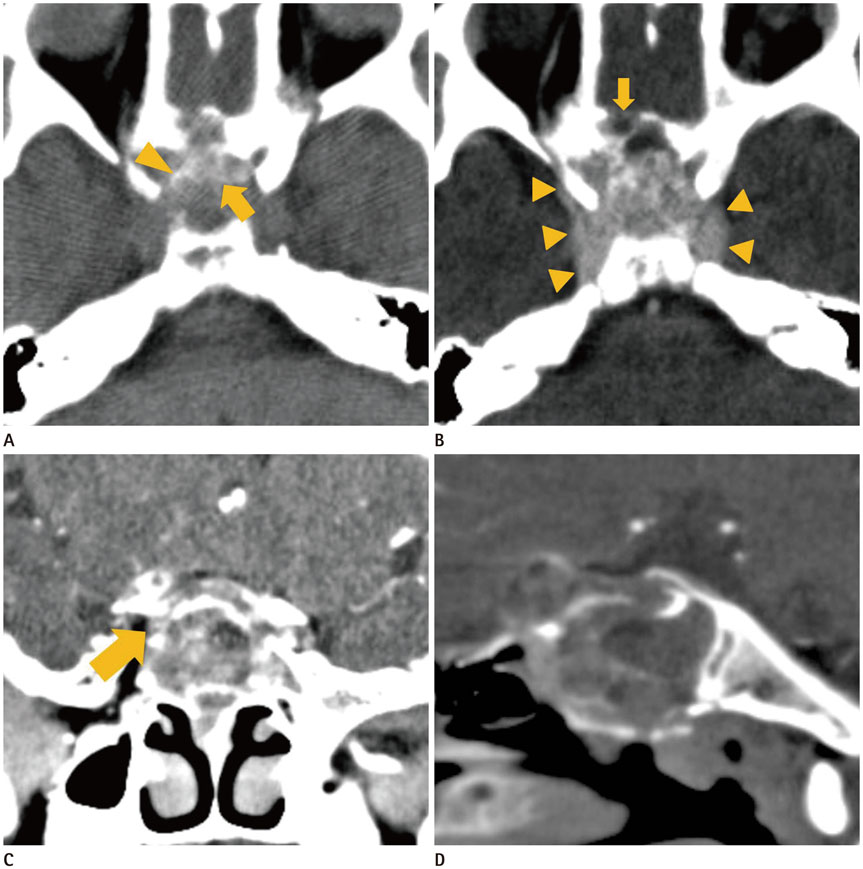
Fig. 1 CT images of chondroblastoma with secondary aneurysmal bone cyst in the sphenoid sinus in a 13-year-old boy. A. On pre-contrast axial plane image, a localized multilobulated, multiseptated small cystic mass (about 35 × 40 × 40 mm in size) involving the both sphenoid sinuses, posterior ethmoid sinuses, both frontal bases, right optic foramen, and right anterior cavernous sinus area is observed. High-attenuation lesion suggesting hemorrhage (arrow, about 40 HU) is observed inside the mass. A few foci of calcification (arrowhead, about 140 HU) are identified both inside the lesion and on the periphery of the lesion. B. The mass shows heterogeneous enhancement on post-contrast CT image. Note that the lateral border of the tumor (arrowheads) is well delineated; however, the anterior border (arrow) is ambiguous on CT. C. On post-contrast enhanced coronal plane image, the mass involves the sphenoid sinus and sellar floor. Extension into the right optic foramen (arrow) is suspected, but not obvious. D. On a bone window setting, bony erosion of the ethmoid roof and sellar floor is well visualized. HU = Hounsfield unit
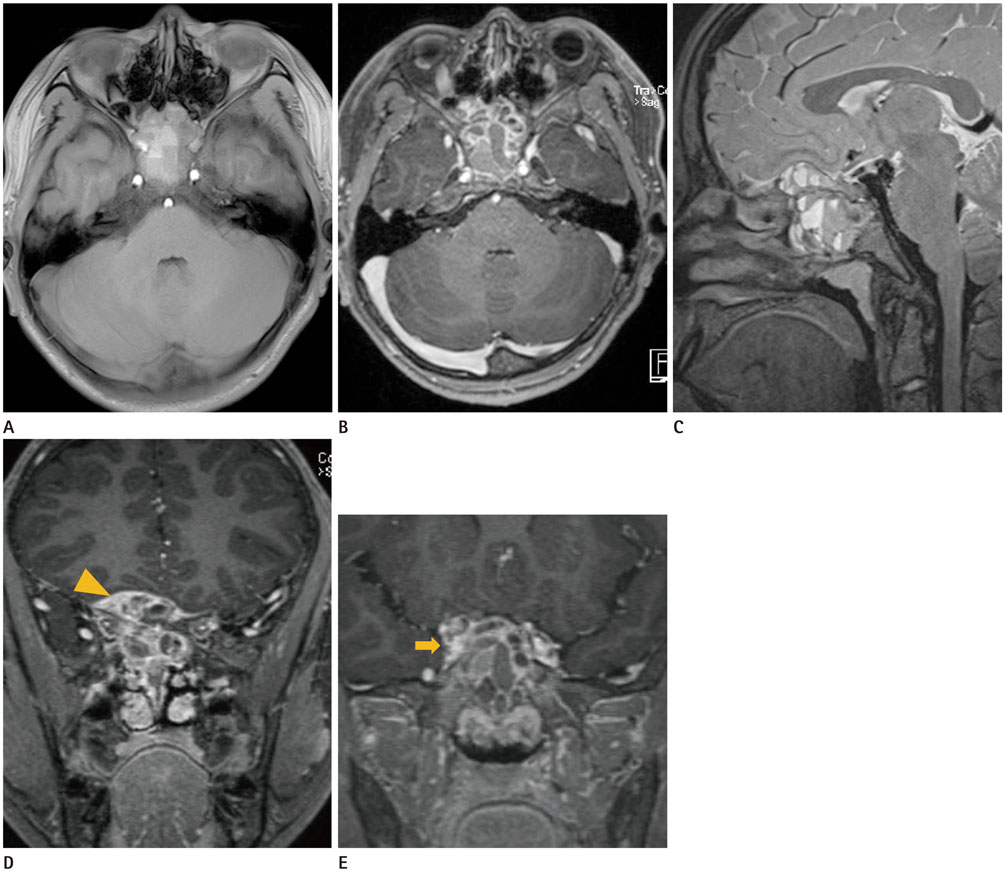
Fig. 2 MR images of the same patient. A. On axial T1-weighted image, a multilobulated and multiseptated small cystic mass involving the sphenoid sinus, both posterior ethmoid sinuses, both frontal bases, and right optic foramen is observed. The mass shows intermediate to high T2 signal intensity. B. On axial post-contrast enhanced T1-weighted image, solid portion of the mass including multiple septa shows good enhancement. C. Fluid-fluid levels in the mass suggesting aneurysmal bone cyst are identified on sagittal T2-weighted image. D. A focal prominent thickened enhancing portion (arrowhead) in the right frontal base is visualized on coronal post-contrast T1-weighted image. The lesion was considered direct dural invasion. E. On coronal post-contrast enhanced T1-weighted image, the mass shows direct invasion into the right anterior cavernous sinus (arrow). MR = magnetic resonance
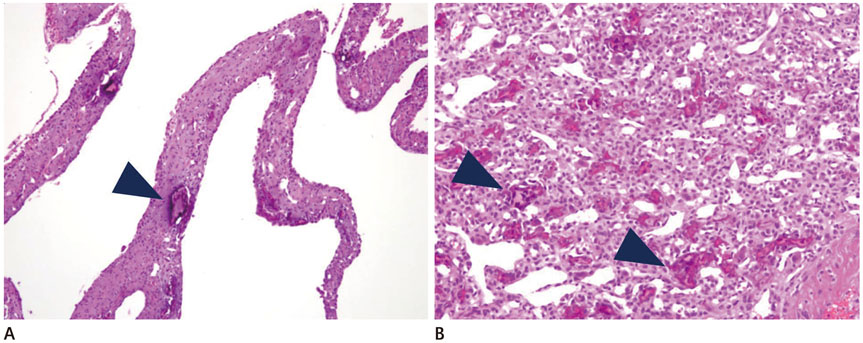
Fig. 3 Pathological examination of the surgical specimen show typical chondroblastoma with secondary aneurysmal bone cyst. A. A low-power magnification view shows fibrous septa and cystic walls that are present in the cystic mass. Cystic walls and septae are lined by fibroblasts, myofibroblasts, and histiocytes. Degenerated calcifying fibromyxoid tissue (arrowhead) is present in loose spindly stroma to cellular stroma. This cystic portion is the secondary aneurysmal bone cyst component of the main tumor (H&E, × 40). B. At higher magnification of the chondroblastoma component, the characteristic fine network of pericellular “chicken wire” calcification is seen. The characteristic cells having a uniform, round to polygonal shape with well-defined cell borders, slightly clear cytoplasm, and a round to ovoid nucleus are seen in cellular sheets. Also, osteoclast-like giant cells (arrowheads) are randomly distributed in the stroma (H&E, × 200). H&E = hematoxylin and eosin
Reference
-
1. Stapleton CJ, Walcott BP, Linskey KR, Kahle KT, Nahed BV, Asaad WF. Temporal bone chondroblastoma with secondary aneurysmal bone cyst presenting as an intracranial mass with clinical seizure activity. J Clin Neurosci. 2011; 18:857–860.2. Kricun ME, Kricun R, Haskin ME. Chondroblastoma of the calcaneus: radiographic features with emphasis on location. AJR Am J Roentgenol. 1977; 128:613–616.3. Muntané A, Valls C, Angeles de Miquel MA, Pons LC. Chondroblastoma of the temporal bone: CT and MR appearance. AJNR Am J Neuroradiol. 1993; 14:70–71.4. Patrocínio TG, Patrocínio LG, de Castro SC, Souza AD, Patrocínio JA. Chondroblastoma of the sphenoid bone. Intl Arch Otorhinolaryngol. 2008; 12:579–581.5. Wang MJ, Zhou B. Chondroblastoma with secondary aneurysmal bone cyst in the anterior skull base. Interdiscip Neurosurg. 2016; 4:13–16.6. Erickson JK, Rosenthal DI, Zaleske DJ, Gebhardt MC, Cates JM. Primary treatment of chondroblastoma with percutaneous radio-frequency heat ablation: report of three cases. Radiology. 2001; 221:463–468.7. Brower AC, Moser RP, Kransdorf MJ. The frequency and diagnostic significance of periostitis in chondroblastoma. AJR Am J Roentgenol. 1990; 154:309–314.8. Weatherall PT, Maale GE, Mendelsohn DB, Sherry CS, Erdman WE, Pascoe HR. Chondroblastoma: classic and confusing appearance at MR imaging. Radiology. 1994; 190:467–474.9. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. Aneurysmal bone cyst: a review of 150 patients. J Clin Oncol. 2005; 23:6756–6762.10. Ramappa AJ, Lee FY, Tang P, Carlson JR, Gebhardt MC, Mankin HJ. Chondroblastoma of bone. J Bone Joint Surg Am. 2000; 82-A:1140–1145.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chondroblastoma of the Talus Mimicking an Aneurysmal Bone Cyst: A Case Report
- Secondary Aneurysmal Bone Cystic Change of the Chondroblastoma, Mistaken for a Primary Aneurysmal Bone Cyst in the Patella
- Aneurysmal Bone Cyst in Clavicle: Report of A Case
- A Case of Aneurysmal Bone Cyst in the Skull Base
- Chondroblastoma of the patella: a case report
