Real-Time Detection of Cerebral Artery Rebleeding by Transcranial Doppler Ultrasound: Hemodynamic Changes and Response to Treatment
- Affiliations
-
- 1Department of Neurology, Henry Ford Hospital, Detroit, MI, USA.
- 2Department of Neurosurgery, Henry Ford Hospital, Detroit, MI, USA.
- 3Second Department of Neurology, School of Medicine, University of Athens, Athens, Greece. tsivgoulisgiorg@yahoo.gr
- KMID: 2364909
- DOI: http://doi.org/10.3988/jcn.2017.13.1.109
Abstract
- No abstract available.
Figure
-
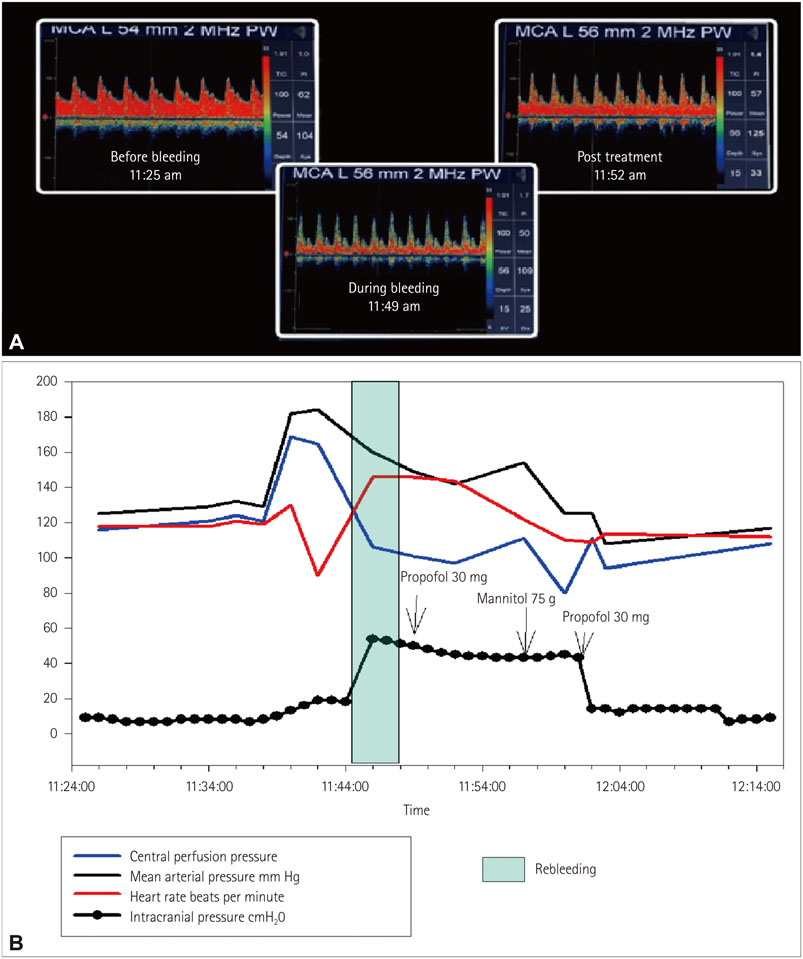
Fig. 1 A: TCD waveforms before, during the bleed and post treatment (A and B left middle cerebral artery). Prior to bleed: ICP was 8 mm Hg, left MCA flow velocity was 61 cm/sec and PI was 1.0. During bleed: ICP increased to 54 mm Hg and PI to 1.7, with the waveform showing a narrow peak and decreased diastolic and mean velocity. 75 g of mannitol was given and the ventriculostomy was opened to drain. Within 5 minutes the ICP decreased to 14, PI improved to 1.4, the waveform widened and the velocities returned to previous levels. Please also see supplemental video. B: Telemetry data, mean arterial pressure increased and cerebral perfusion pressure increased before the rebleed. During rebleed there was a trend for ICP elevation (up to 54 mm Hg, but with poor waveform). After therapy with propofol and mannitol all normalized. ICP: intracranial pressure, MCA: middle cerebral artery, PI: pulsatility index, TCD: Transcranial Doppler ultrasound.
Reference
-
1. Fugate JE, Rabinstein AA. Intensive care unit management of aneurysmal subarachnoid hemorrhage. Curr Neurol Neurosci Rep. 2012; 12:1–9.
Article2. Rowland MJ, Hadjipavlou G, Kelly M, Westbrook J, Pattinson KT. Delayed cerebral ischaemia after subarachnoid haemorrhage: looking beyond vasospasm. Br J Anaesth. 2012; 109:315–329.
Article3. Alexandrov AV, Sloan MA, Tegeler CH, Newell DN, Lumsden A, Garami Z, et al. Practice standards for transcranial Doppler (TCD) ultrasound. Part II. Clinical indications and expected outcomes. J Neuroimaging. 2012; 22:215–224.
Article4. Plesnila N. Pathophysiological role of global cerebral ischemia following subarachnoid hemorrhage: the current experimental evidence. Stroke Res Treat. 2013; 2013:651958.
Article5. Ohkuma H, Tsurutani H, Suzuki S. Incidence and significance of early aneurysmal rebleeding before neurosurgical or neurological management. Stroke. 2001; 32:1176–1180.
Article6. Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009; 40:994–1025.
Article7. Lin QS, Ping-Chen , Lin YX, Lin ZY, Yu LH, Dai LS, et al. Systolic blood pressure variability is a novel risk factor for rebleeding in acute subarachnoid hemorrhage: a case-control study. Medicine (Baltimore). 2016; 95:e3028.8. Sun Y, Shen Q, Watts LT, Muir ER, Huang S, Yang GY, et al. Multimodal MRI characterization of experimental subarachnoid hemorrhage. Neuroscience. 2016; 316:53–62.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Implications of a Variation of Middle Cerebral Artery in the Interpretation of Transcranial Doppler
- Changes in Interictal Cerebral Blood Flow in Patients with Epilepsy
- Effect of Calculation Task on the Regional Cerebral Blood Flow Velocity: a Transcranial Doppler Study
- Transcranial Doppler Sonography in Acute Ischemic Stroke
- Hemodynamic Infarction Associated with Coil Embolization of Intracranial Aneurysm
