Gardner syndrome associated with multiple osteomas, intestinal polyposis, and epidermoid cysts
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, School of Dentistry and Institute of Oral Bioscience, Chonbuk National University, Jeonju-si, Republic of Korea. kkj1512@jbnu.ac.kr
- KMID: 2362745
- DOI: http://doi.org/10.5624/isd.2016.46.4.267
Abstract
- Gardner syndrome is known as a variant of familial adenomatous polyposis. This syndrome is characterized by multiple intestinal polyposes, osteomas, and epidermoid cysts. In addition, dental abnormalities include an increased frequency of multiple odontomas, as well as supernumerary and impacted teeth. The authors report the case of a 7-year-old male patient with Gardner syndrome. Radiographic findings revealed multiple osteomas in both sides of the maxilla, multiple diffuse enostoses in both jaws, and a complex odontoma in the left mandibular body. Two years later, multiple epidermoid cysts on the scalp were found. Since this patient was suspected to have Gardner syndrome, the authors recommended gastrointestinal endoscopy to check for intestinal polyposis. Gastrointestinal endoscopic examination revealed multiple polyposes in the upper gastrointestinal tract and fundus of the stomach. As a result, the final diagnosis was Gardner syndrome.
MeSH Terms
Figure
-
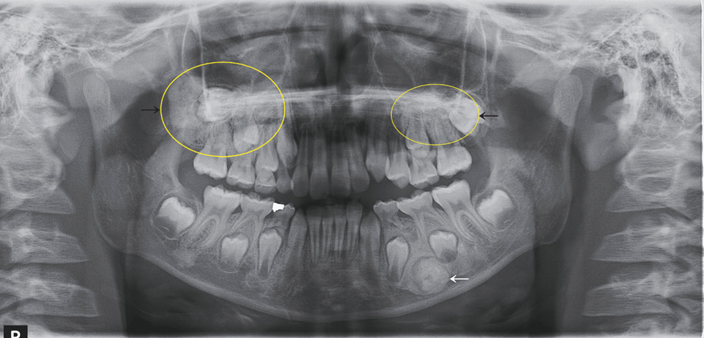
Fig. 1 A panoramic image shows relatively well-defined multiple radiopacities in both maxillary posterior regions encroaching the maxillary sinuses (black arrows), a well-defined round radiopacity surrounded with a radiolucent line in the left mandibular premolar area (white arrow), and multiple diffuse radiopacities in both jaws.

Fig. 2 A post-enhanced coronal computed tomography image shows multiple mildly enhanced soft tissue masses on the subcutaneous areas of the scalp.
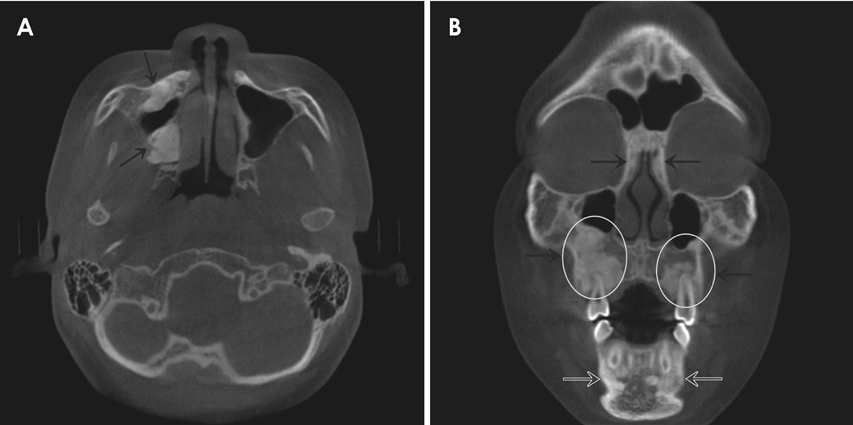
Fig. 3 A. An axial cone-beam computed tomography (CBCT) image shows multiple radiopaque masses in the right maxilla encroaching the maxillary sinus (black arrows). B. A coronal CBCT image shows multiple diffuse radiopacities in the mandible (white open arrows), and multiple radiopacities encroaching the maxillary sinuses and ethmoidal sinuses (black arrows).

Fig. 4 A photograph of the patient's scalp shows multiple nodules on the scalp.

Fig. 5 Histopathologic examination of the nodules on the scalp shows a cystic wall with lining epithelium (H&E stain, ×200).

Fig. 6 A. An endoscopic examination shows multiple polyposes on the upper gastrointestinal tract. B. Endoscopic examination showing multiple polyposes on the fundus of the stomach.

Fig. 7 A. A photomicrograph of the decalcified section of the radiopaque mass in right maxillary posterior region shows dense and lamellar cortical bone with narrow bone marrow spaces (H&E stain, ×50). B. A photomicrograph of the decalcified section of radiopaque mass in the left mandibular body shows irregularly deposited cementum, dentin, and enamel matrix (H&E stain, ×50).
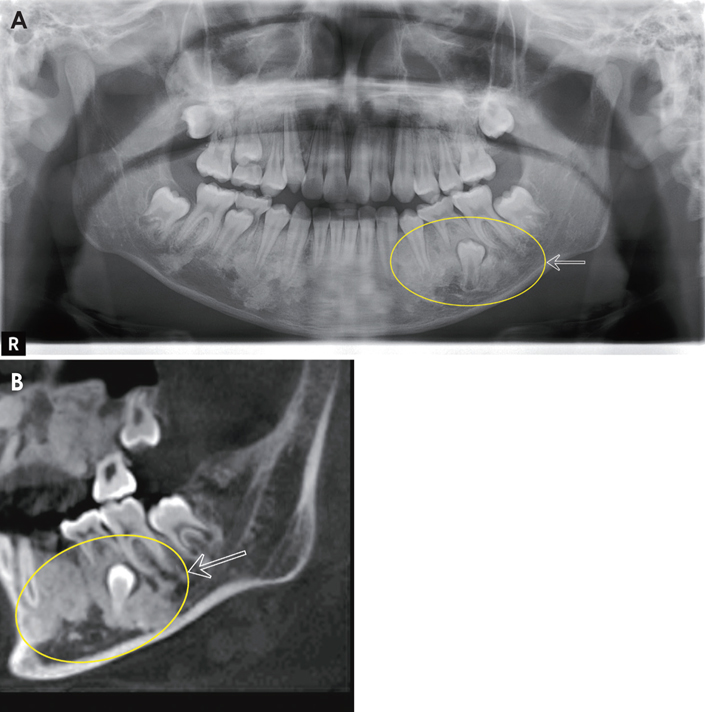
Fig. 8 A. Two years after removal of the complex odontoma in the left mandibular body and osteoma in the right tuberosity, a panoramic image shows the remaining radiopaque lesions in both sides of the maxilla and diffuse enostoses in both jaws (white open arrow). B. A sagittal cone-beam computed tomography image shows multiple enostoses with impaction of the left mandibular second premolar (white open arrow).
Cited by 1 articles
-
Clinicopathologic features of epidermoid cysts in the upper and lower extremities, including a case of malignant transformation in the palmoplantar region
Sungmi Jeon, Se Yeon Lee, Jinhyun Kim, Ung Sik Jin, Sung Tack Kwon, Yoonjin Kwak, Byung Jun Kim
Arch Hand Microsurg. 2022;27(4):285-291. doi: 10.12790/ahm.22.0049.
Reference
-
1. Herrmann SM, Adler YD, Schmidt-Petersen K, Nicaud V, Morrison C, Paul M, et al. The concomitant occurrence of multiple epidermal cysts, osteomas and thyroid gland nodules is not diagnostic for Gardner syndrome in the absence of intestinal polyposis: a clinical and genetic report. Br J Dermatol. 2003; 149:877–883.
Article2. Tan KL, Wilson S, O'Neill C, Gordon D, Napier S. Something not quite right: Gardner syndrome diagnosed by multiple cutaneous lesions and genetic testing. Surgeon. 2005; 3:412–415.
Article3. Fearnhead NS, Britton MP, Bodmer WF. The ABC of APC. Hum Mol Genet. 2001; 10:721–733.
Article4. Ramaglia L, Morgese F, Filippella M, Colao A. Oral and maxillofacial manifestations of Gardner's syndrome associated with growth hormone deficiency: case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e30–e34.
Article5. Perniciaro C. Gardner's syndrome. Dermatol Clin. 1995; 13:51–56.
Article6. Herford AS, Stoffella E, Tandon R. Osteomas involving the facial skeleton: a report of 2 cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 115:e1–e6.
Article7. Chimenos-Küstner E, Pascual M, Blanco I, Finestres F. Hereditary familial polyposis and Gardner's syndrome: contribution of the odonto-stomatology examination in its diagnosis and a case description. Med Oral Patol Oral Cir Bucal. 2005; 10:402–409.8. Ida M, Nakamura T, Utsunomiya J. Osteomatous changes and tooth abnormalities found in the jaw of patients with adenomatosis coli. Oral Surg Oral Med Oral Pathol. 1981; 52:2–11.9. Butler J, Healy C, Toner M, Flint S. Gardner syndrome - review and report of a case. Oral Oncol Extra. 2005; 41:89–92.10. Lew D, DeWitt A, Hicks RJ, Cavalcanti MG. Osteomas of the condyle associated with Gardner's syndrome causing limited mandibular movement. J Oral Maxillofac Surg. 1999; 57:1004–1009.
Article11. Bilkay U, Erdem O, Ozek C, Helvaci E, Kilic K, Ertan Y, et al. Benign osteoma with Gardner syndrome: review of the literature and report of a case. J Craniofac Surg. 2004; 15:506–509.
Article12. Lee BD, Lee W, Oh SH, Min SK, Kim EC. A case report of Gardner syndrome with hereditary widespread osteomatous jaw lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:e68–e72.
Article13. Wolf J, Jarvinen HJ, Hietanen J. Gardner's dento-maxillary stigmas in patients with familial adenomatosis coli. Br J Oral Maxillofac Surg. 1986; 24:410–416.
Article14. Carl W, Sullivan MA. Dental abnormalities and bone lesions associated with familial adenomatous polyposis: report of cases. J Am Dent Assoc. 1989; 119:137–139.
Article15. Cankaya AB, Erdem MA, Isler SC, Cifter M, Olgac V, Kasapoglu C, et al. Oral and maxillofacial considerations in Gardner's syndrome. Int J Med Sci. 2012; 9:137–141.
Article16. Ortakoglu K, Gunaydin Y, Aydintug YS, Safali M. Osteoma of the mandibular condyle: report of a case with 5-year follow-up. Mil Med. 2005; 170:117–120.17. Fonseca LC, Kodama NK, Nunes FC, Maciel PH, Fonseca FA, Roitberg M, et al. Radiographic assessment of Gardner's syndrome. Dentomaxillofac Radiol. 2007; 36:121–124.
Article18. Madani M, Madani F. Gardner's syndrome presenting with dental complaints. Arch Iran Med. 2007; 10:535–539.19. Melrose RJ, Abrams AM, Mills BG. Florid osseous dysplasia. A clinical-pathologic study of thirty-four cases. Oral Surg Oral Med Oral Pathol. 1976; 41:62–82.20. Waldron C. Bone pathology. Oral and maxillofacial pathology. Philadelphia: WB Saunders Comp;1995. p. 460–491.
