Treatment of Acute Retinal Necrosis with Acute Kidney Injury after Intravenous Antiviral Injection
- Affiliations
-
- 1Department of Ophthalmology, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea. Syu2000@hanmail.net
- KMID: 2362719
- DOI: http://doi.org/10.3341/jkos.2016.57.12.1976
Abstract
- PURPOSE
In the present study, a case of acute retinal necrosis with acute renal injury due to high-dose intravenous antiviral injection which was treated by intravitreal ganciclovir injection is reported.
CASE SUMMARY
A 46-year-old female visited our clinic complaining of red eye and decreased vision in the right eye. At the first visit, her corrected visual acuity was finger count in the right eye, and 20/20 in the left eye. Fundus examination of the right eye revealed multiple peripheral arterial occlusion, papilledema, and whitish necrotic infiltration at the periphery. Clinically diagnosed as acute retinal necrosis, the patient was started on intravenous acyclovir. Two days after injection, her serum creatinine level increased, therefore, intravenous acyclovir was discontinued and she was started on intravitreal ganciclovir. Five days after the intravenous injection was discontinued, the serum creatinine level returned to normal range. Four months after the first visit, visual acuity was 20/100 and no recurrence was observed.
CONCLUSIONS
Intravitreal ganciclovir injection can be an effective alternative in patients with acute retinal necrosis and poor kidney function.
MeSH Terms
Figure
-

Figure 1. Fundus photograph and fluorescein angiography at initial visit. Confluent, whitish, and necrotic infiltrations are seen around peripheral retina. Obstructive arteritis, vitreous haziness and disc edema are also observed.
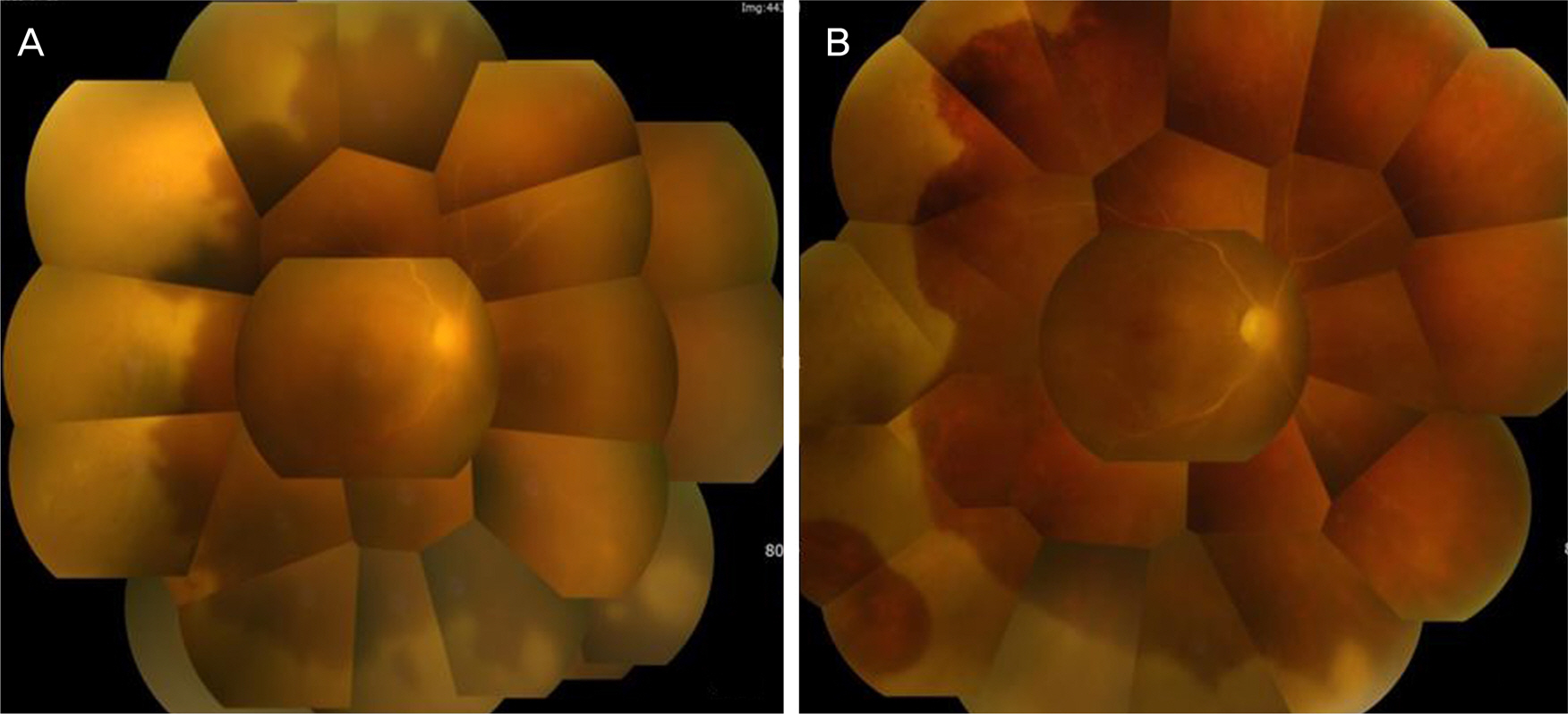
Figure 2. Fundus photographs after administration. (A) Hospital day #2. After intravenous acyclovir, the progression of the diseases was stopped, however, acyclovir-induced acute renal injury was occurred. (B) Hospital day #7. Instead of IV acyclovir, intravitreal gancyclovir was performed 2 times per week. The area of infiltrations began to decrease.
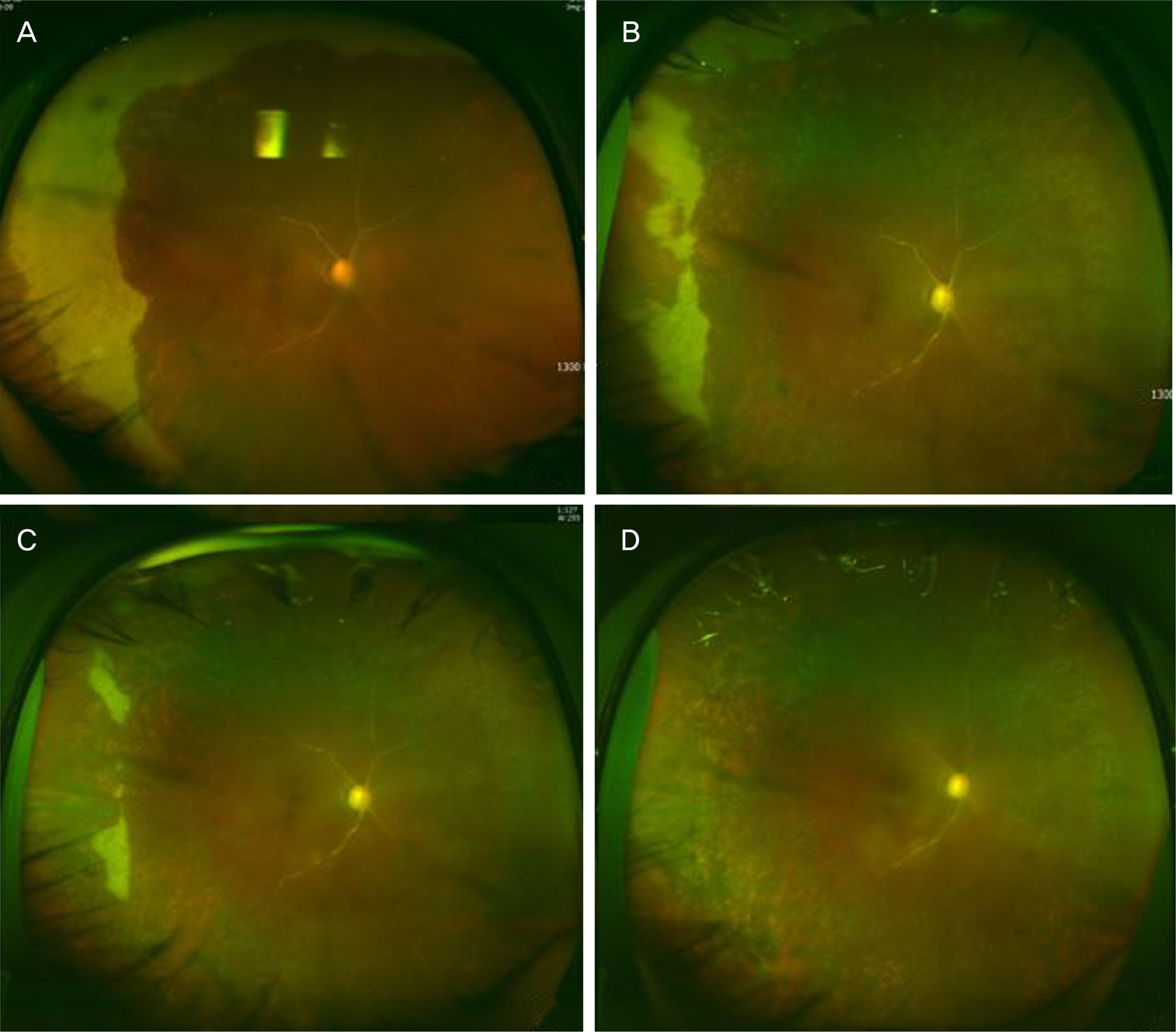
Figure 3. Chronologic order of ultrawide fundus images during the patient's clinical course. (A) One month after initial visit. Peripheral confluent whitish lesions were moved to more peripheral area. At that time, 360° barrier laser was done. 6 week (B) and 8 weeks (C) later, peripheral infiltrations were significantly improved. 3 months later (D), no infiltration was observed.
Reference
-
References
1. Lau CH, Missotten T, Salzmann J, Lightman SL. Acute retinal abdominal features, management, and outcomes. Ophthalmology. 2007; 114:756–62.2. Holland GN. Standard diagnostic criteria for the acute retinal syndrome. Executive Committee of the American Uveitis Society. Am J Ophthalmol. 1994; 117:663–7.3. Clarkson JG, Blumenkranz MS, Culbertson WW, et al. Retinal abdominal following the acute retinal necrosis syndrome. Ophthalmology. 1984; 91:1665–8.4. Freeman WR, Thomas EL, Rao NA, et al. Demonstration of herpes group virus in acute retinal necrosis syndrome. Am J Ophthalmol. 1986; 102:701–9.
Article5. de Boer JH, Verhagen C, Bruinenberg M, et al. Serologic and abdominal chain reaction analysis of intraocular fluids in the diagnosis of infectious uveitis. Am J Ophthalmol. 1996; 121:650–8.6. Chau Tran TH, Cassoux N, Bodaghi B, Lehoang P. Successful treatment with combination of systemic antiviral drugs and abdominal ganciclovir injections in the management of severe abdominal herpetic retinitis. Ocul Immunol Inflamm. 2003; 11:141–4.7. Mastsuo T. Vitrectomy and silicone oil tamponade as an initial abdominal for retinal detachment after acute retinal necrosis syndrome. Ocul Immunol Inflamm. 2005; 13:91–4.8. McDonald HR, Lewis H, Kreiger AE, et al. Surgical management of retinal detachment associated with the acute retinal necrosis syndrome. Br J Ophthalmol. 1991; 75:455–8.
Article9. Duker JS, Blumenkranz MS. Diagnosis and management of the acute retinal necrosis (ARN) syndrome. Surv Ophthalmol. 1991; 35:327–43.
Article10. Markowitz GS, Perazella MA. Drug-induced renal failure: a focus on tubulointerstitial disease. Clin Chim Acta. 2005; 351:31–47.
Article11. Bean B, Aeppli D. Adverse effects of high-dose intravenous abdominal in ambulatory patients with acute herpes zoster. J Infect Dis. 1985; 151:362–5.12. Cho JH, Jang JH, Lee DH, et al. Acyclovir-induced acute renal abdominal in a patient with suspected acute retinal necrosis syndrome. J Korean Ophthalmol Soc. 2010; 51:1528–31.13. Wong RW, Jumper JM, McDonald HR, et al. Emerging concepts in the management of acute retinal necrosis. Br J Ophthalmol. 2013; 97:545–52.
Article14. Emerson GG, Smith JR, Wilson DJ, et al. Primary treatment of acute retinal necrosis with oral antiviral therapy. Ophthalmology. 2006; 113:2259–61.
Article15. Liu DT, Lee VY, Lam PT, Lam DS. Acyclovir-induced nephroabdominal in a patient with acute retinal necrosis. Hong Kong Med J. 2007; 13:155–6.16. Yang JW, Kim WJ, Park YH. Two cases of acute retinal necrosis treated with systemic antiviral drugs and intravitreal antiviral injections. J Korean Ophthalmol Soc. 2009; 50:794–9.
Article17. Yeh S, Suhler EB, Smith JR, et al. Combination systemic and abdominal antiviral therapy in the management of acute retinal necrosis syndrome. Ophthalmic Surg Lasers Imaging Retina. 2014; 45:399–407.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Acute Retinal Necrosis Treated With Systemic Antiviral Drugs and Intravitreal Antiviral Injections
- Acute Retinal Necrosis Syndrome in an Immunosuppressed Kidney Transplant Patient
- Vitrectomy and Silicone Oil Tamponade to Prevent Retinal Detachment in Severe Acute Retinal Necrosis Syndrome
- Acyclovir-induced Acute Renal Failure in a Patient With Suspected Acute Retinal Necrosis Syndrome
- Presumed Necrotizing Viral Retinitis after Intravitreal Triamcinolone Injection: Case Report
