Comparison of Clinical Outcomes between Laser Blended Vision and Monovision Laser Refractive Surgery for Presbyopia
- Affiliations
-
- 1HanGil Eye Hospital, Incheon, Korea. chobjn@empas.com
- KMID: 2362700
- DOI: http://doi.org/10.3341/jkos.2016.57.12.1840
Abstract
- PURPOSE
To compare the efficacy and safety of Laser Blended Vision (LBV) and monovision laser refractive surgery (monovision) for presbyopia correction in patients with myopia.
METHODS
This retrospective comparative study included 42 eyes of 21 patients with LBV and 50 eyes of 25 patients with monovision. Monocular and binocular distance, intermediate and near visual acuity, and refractive changes were evaluated preoperatively and 3 months after the surgery and compared. The patients in the LBV group underwent further evaluation of spherical aberration 3 months after the surgery and treatment satisfaction 3-6 months after the surgery.
RESULTS
The mean age of the patients was 47.9 years in the LBV group and 41.7 years in the monovision group. Three months after surgery, the spherical equivalents were +0.11 ± 0.17 D in the dominant eye and -1.52 ± 0.36 D in the non-dominant eye in the LBV group. In contrast, the spherical equivalents were +0.23 ± 0.26 D in the dominant eye and -0.82 ± 0.28 D in the non-dominant eye in the monovision group. All patients achieved a binocular uncorrected distance visual acuity of 0.10 (log MAR) or better, and 86% of the LBV group and 100% of the monovision group achieved a binocular uncorrected intermediate visual acuity of better than 0.10. Moreover, 95% of the LBV group and 100% of the monovision group achieved a binocular uncorrected near visual acuity of better than 0.18. In the LBV group, mean spherical aberration increased after surgery than before, but it was not statistically significant. Complications such as corneal opacity that could decrease visual acuity were absent in both groups. Overall patient satisfaction after surgery was 80% in the LBV group.
CONCLUSIONS
Despite the relatively higher mean age of the LBV group, both groups showed similar results regarding presbyopia correction in patients with myopia.
Keyword
MeSH Terms
Figure
-
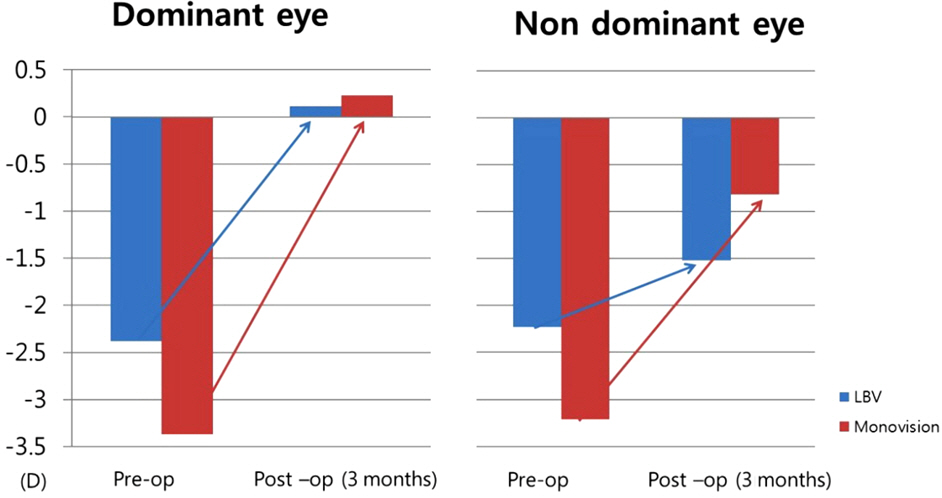
Figure 1. Refractive change in laser blended vision (LBV) and monovision. Preoperation and 3 months after surgery. Pre-op = preoperation; Post-op = preoperation.
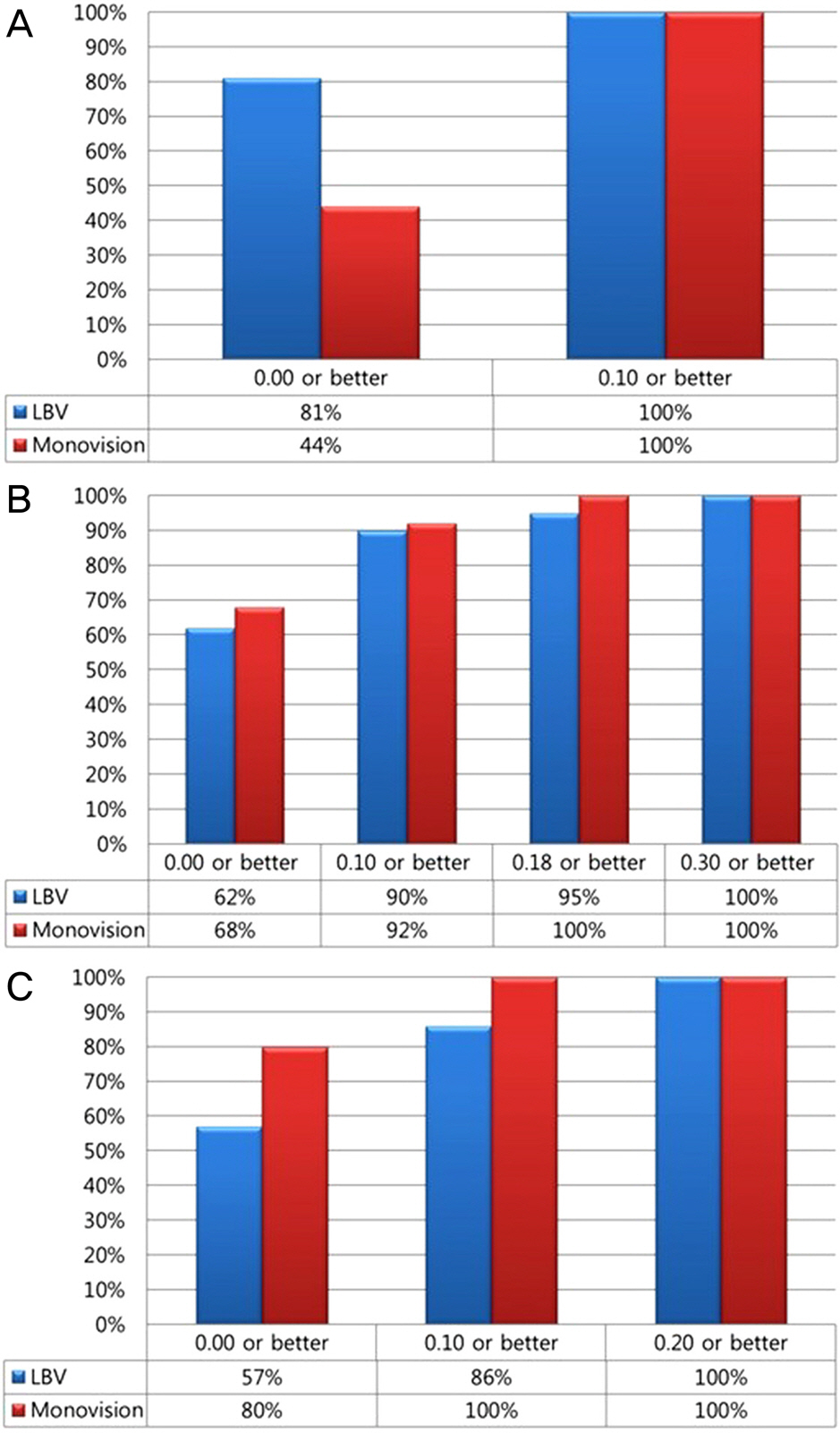
Figure 2. Cumulative histogram of visual acuity after laser blended vision (LBV) and monovision. (A) Uncorrected distance visual acuity. (B) Uncorrected near visual acuity. (C) Uncorrected intermediate visual acuity.

Figure 3. Comparison between laser blended vision (LBV) and monovision. (A) Binocular visual acuity. There was no statistically significant difference in distance, intermediate, and near visual acuity. (B) Dominant eye visual acuity. Monovision had better near visual acuity. (C) Non-dominant eye visual acuity. There was no statistically significant difference in distance, intermediate, and near visual acuity. UDVA = uncorrected distance visual acuity at 4 m; UIVA = uncorrected intermediate visual acuity at 80 cm; UNVA = uncorrected near visual acuity at 33–40 cm. * p-value was acquired from Mann-Whitney U-test.
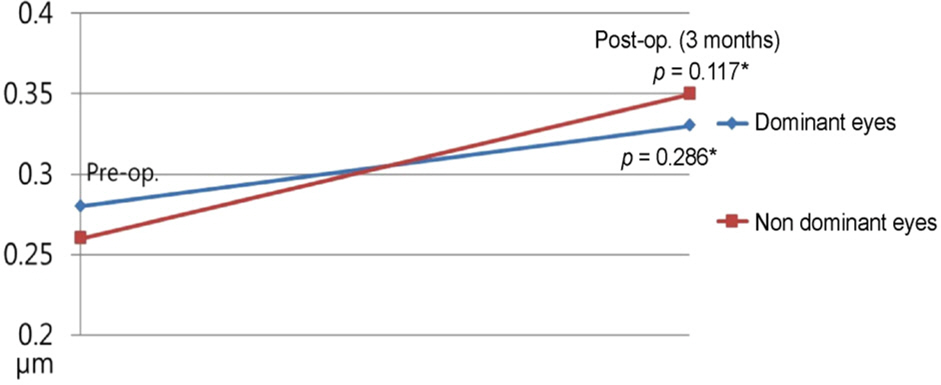
Figure 4. Corneal spherical aberration of laser blended vision. At 3 months postoperatively, spherical aberration increased in non dominant and dominant eye. Pre-op = preoperation; Post-op = postoperation. * p-value was acquired from Wilcoxon signed rank test.
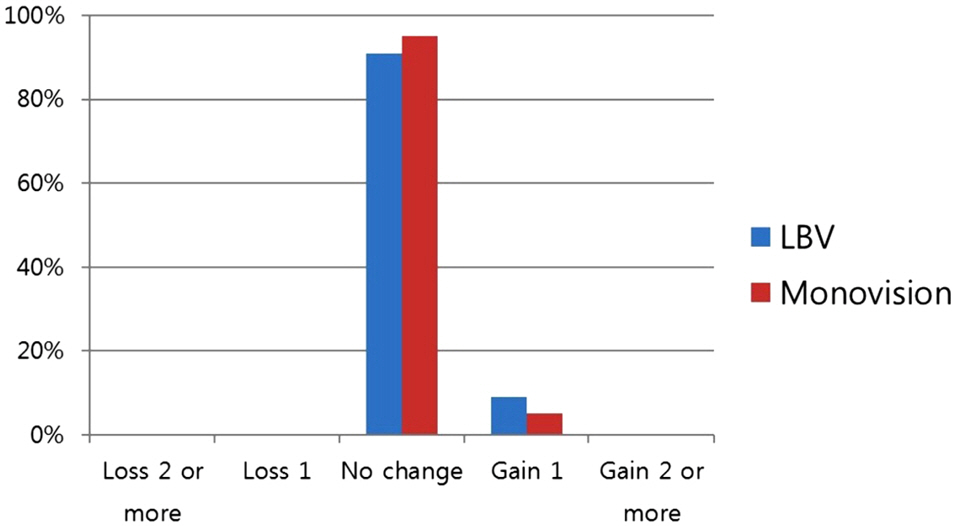
Figure 5. Safety: changes of postoperative best corrected distant visual acuity. There was no visual loss at 3 months postoperatively. LBV = laser blended vision.
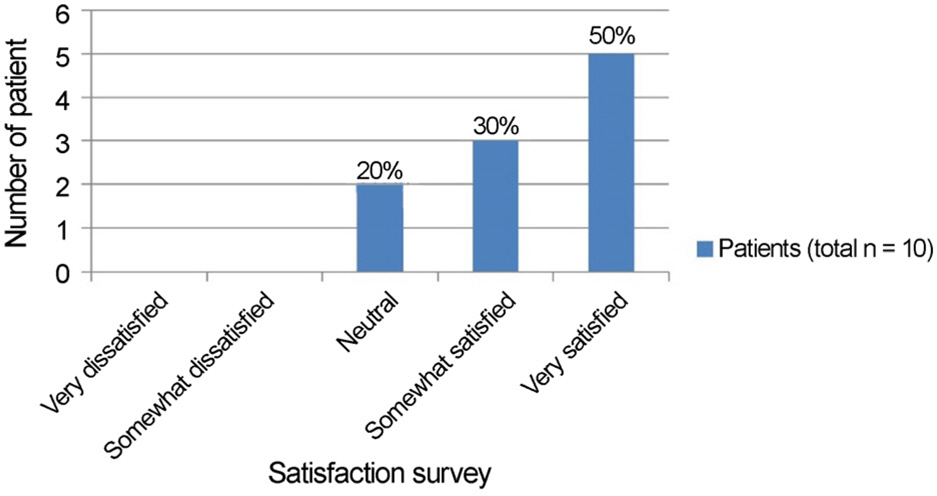
Figure 6. Overall satisfaction after Laser blended vision. Eighty percent of the patients were satisfied with the results of the operation.
Cited by 1 articles
-
What is presbyopia?
Ji-Won Kwon
J Korean Med Assoc. 2019;62(12):608-610. doi: 10.5124/jkma.2019.62.12.608.
Reference
-
References
1. Oum BS. Eye Exam. 3rd ed.Goyang: Naewaehs;2013. p. 98.2. Duane A. A modified accommodation line and Prince's rule. Trans Am Ophthalmol Soc. 1921; 19:178–9.3. Michaels DD. Visual Optics and Refraction. 1st ed.St. Louis: St. Louis;1975. p. 268–81.4. Beddow DR, Martin SJ, Pfeiffer CH. Presbyopic patients and abdominal vision contact lenses. South J Optom. 1966; 8:9–11.5. Kohnen T, Allen D, Boureau C, et al. European multicenter study of the AcrySof ReSTOR apodized diffractive intraocular lens. Ophthalmology. 2006; 113:584.e1. Epub 2006 Feb 14.
Article6. Heatley CJ, Spalton DJ, Boyce JF, Marshall J. A mathematical model of factors that influence the performance of accommodative intraocular lenses. Ophthalmic Physiol Opt. 2004; 24:111–8.
Article7. Kim YJ, Cheon MH, Ko DA, et al. Visual function and patient abdominal in pseudophakic monovision. J Korean Ophthalmol Soc. 2012; 53:1621–9.8. Waring GO 4th. Correction of presbyopia with a small aperture corneal inlay. J Refract Surg. 2011; 27:842–5.
Article9. Dexl AK, Seyeddain O, Riha W, et al. One-year visual outcomes and patient satisfaction after surgical correction of presbyopia with an intracorneal inlay of a new design. J Cataract Refract Surg. 2011; 38:262–9.
Article10. Harris MG, Classé JG. Clinicolegal considerations of monovision. J Am Optom Assoc. 1988; 59:491–5.11. Stahl JE. Conductive keratoplasty for presbyopia: 3-year results. J Refract Surg. 2007; 23:905–10.
Article12. Goldberg DB. Laser in situ keratomileusis monovision. J Cataract Refract Surg. 2001; 27:1449–55.
Article13. Miranda D, Krueger RR. Monovision laser in situ keratomileusis for pre-presbyopic and presbyopic patients. J Refract Surg. 2004; 20:325–8.
Article14. Reinstein DZ, Archer TJ, Gobbe M. LASIK for myopic abdominal and presbyopia using non-linear aspheric micro-monovision with the Carl Zeiss Meditec MEL 80 platform. J Refract Surg. 2011; 27:23–37.15. Reinstein DZ, Carp GI, Archer TJ, Gobbe M. LASIK for abdominal correction in emmetropic patients using aspheric ablation abdominals and a micro-monovision protocol with the Carl Zeiss Meditec MEL 80 and VisuMax. J Refract Surg. 2012; 28:531–41.16. Goldberg DB. Comparison of myopes and hyperopes after laser in situ keratomileusis monovision. J Cataract Refract Surg. 2003; 29:1695–701.
Article17. Reilly CD, Lee WB, Alvarenga L, et al. Surgical monovision and monovision reversal in LASIK. Cornea. 2006; 25:136–8.
Article18. Braun EH, Lee J, Steinert RF. Monovision in LASIK. Ophthalmology. 2008; 115:1196–202.
Article19. Bae K, Keum JE, Chung TY, Chung ES. LASIK for myopia with presbyopia using the aspheric micro-monovision Technique. J Korean Ophthalmol Soc. 2012; 53:11–9.
Article20. Kang KM, Jung BY, Cho HT, et al. abdominal results of LASIK for presbyopia correction in myopic patients using aspheric mi-cro-monovision. J Korean Ophthalmol Soc. 2013; 54:1893–901.21. Reinstein DZ, Couch DG, Archer TJ. LASIK for Hyperopic abdominal and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 Platform. J Refract Surg. 2009; 25:37–58.22. Chun YS, Lee HI, Dausch D, Kim JC. abdominal results of abdominal corneal surface ablation with Eximer laser. J Korean abdominal Soc. 2008; 49:1061–70.23. Alió JL, Chaubard JJ, Caliz A, et al. Correction of presbyopia by technovision central multifocal LASIK(presbyLASIK). J Refract Surg. 2006; 22:453–60.24. Artola A, Patel S, Schimchak P, et al. Evidence for delayed abdominal after photorefractive keratectomy for myopia. Ophthalmology. 2006; 113:735–41.e1.25. Ares J, Flores R, Bará S, Jaroszewicz Z. Presbyopia compensation with a quartic axicon. Optom Vis Sci. 2005; 82:1071–8.
Article26. Nio YK, Jansonius NM, Wijdh RH, et al. Effect of methods of abdominal correction on visual acuity, contrast sensitivity, and depth of focus. J Cataract Refract Surg. 2003; 29:2082–95.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Evaluationnof Monovision Induced by Laser Thermal Keratoplasty (LTK)
- Surgical treatment of presbyopia I
- Surgical treatment of presbyopia
- Long-Term Results of LASIK for Presbyopia Correction in Myopic Patients Using Aspheric Micro-Monovision
- Clinical Results of Pseudophakic Monovision 1 Year after Cataract Surgery
