Int J Thyroidol.
2016 Nov;9(2):190-194. 10.11106/ijt.2016.9.2.190.
A Case of Methimazole-Resistant Severe Graves' Disease: Dramatic Response to Cholestyramine
- Affiliations
-
- 1Department of Endocrinology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. endo10@daum.net
- KMID: 2362357
- DOI: http://doi.org/10.11106/ijt.2016.9.2.190
Abstract
- A 22-year-old woman with severe Graves' disease was referred from a local clinic because of her refractory hyperthyroidism. She presented with exophthalmos, diffuse goiter, and tachycardia. She was treated with a maximal dose of methimazole and a beta-blocker for 2 months. However, her thyroid function test (TFT) did not improve. TFT showed a free T4 level of 74.7 ng/dL and a thyroid stimulating hormone (TSH) level of 0.007 µIU/mL. She was then administered cholestyramine (4 g thrice daily), hydrocortisone (300 mg/day) and methimazole (100 mg/day) which prepared the patient for surgery by reducing the free T4 level (4.7 ng/dL). The patient underwent a total thyroidectomy without experiencing thyrotoxic crisis. This case describes the use of cholestyramine for the first time in Korea in treating Graves' disease and provides limited evidence that cholestyramine can be an effective option.
Keyword
MeSH Terms
Figure
-

Fig. 1. Patients scintigraphy scan. This shows diffuse enlargement of both lobes of the thyroid gland with increased Tc-99m uptake.
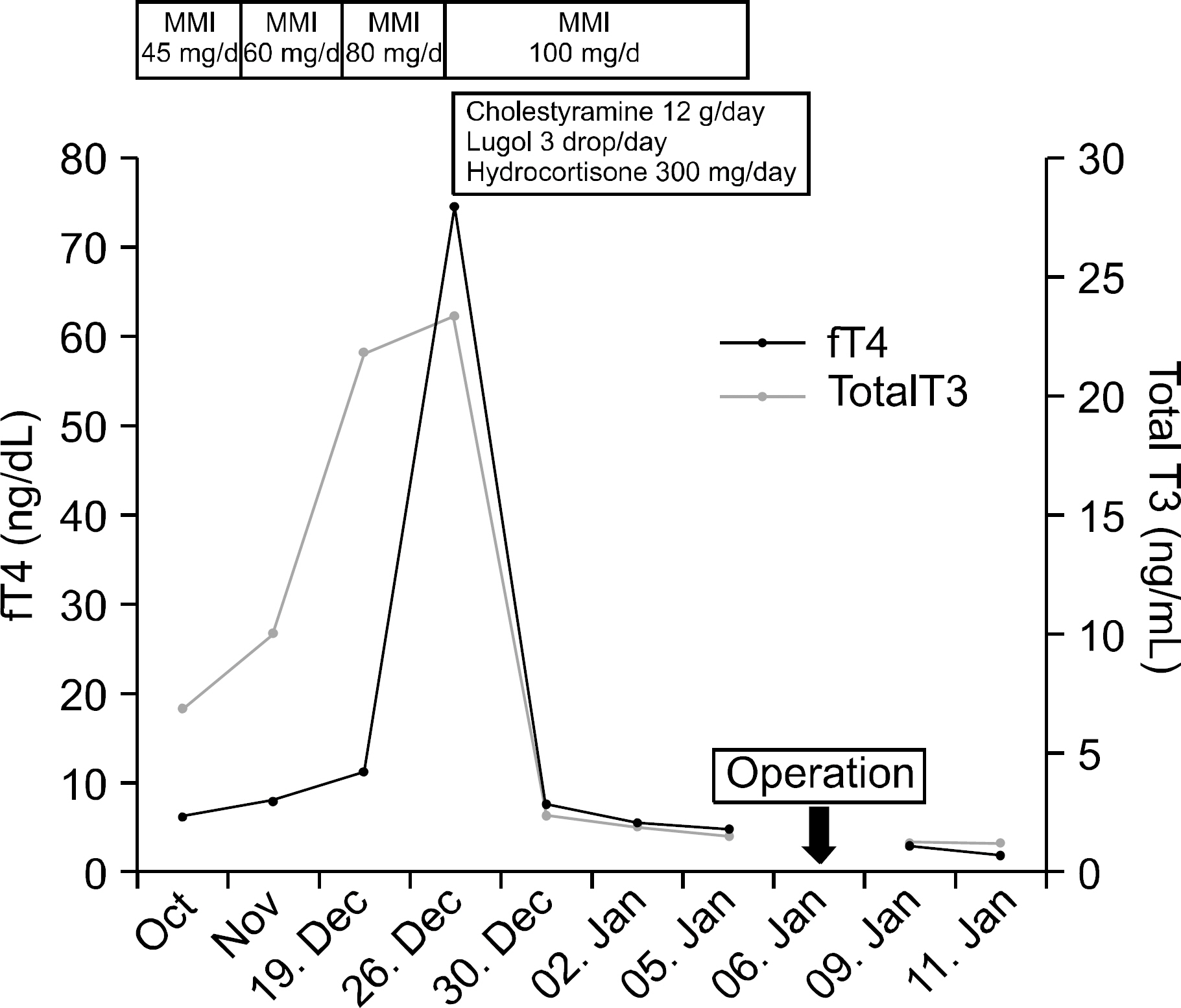
Fig. 2. Interval change of free T4 level and total T3 level following administration of medications (fT4: free T4, MMI: methimazole).
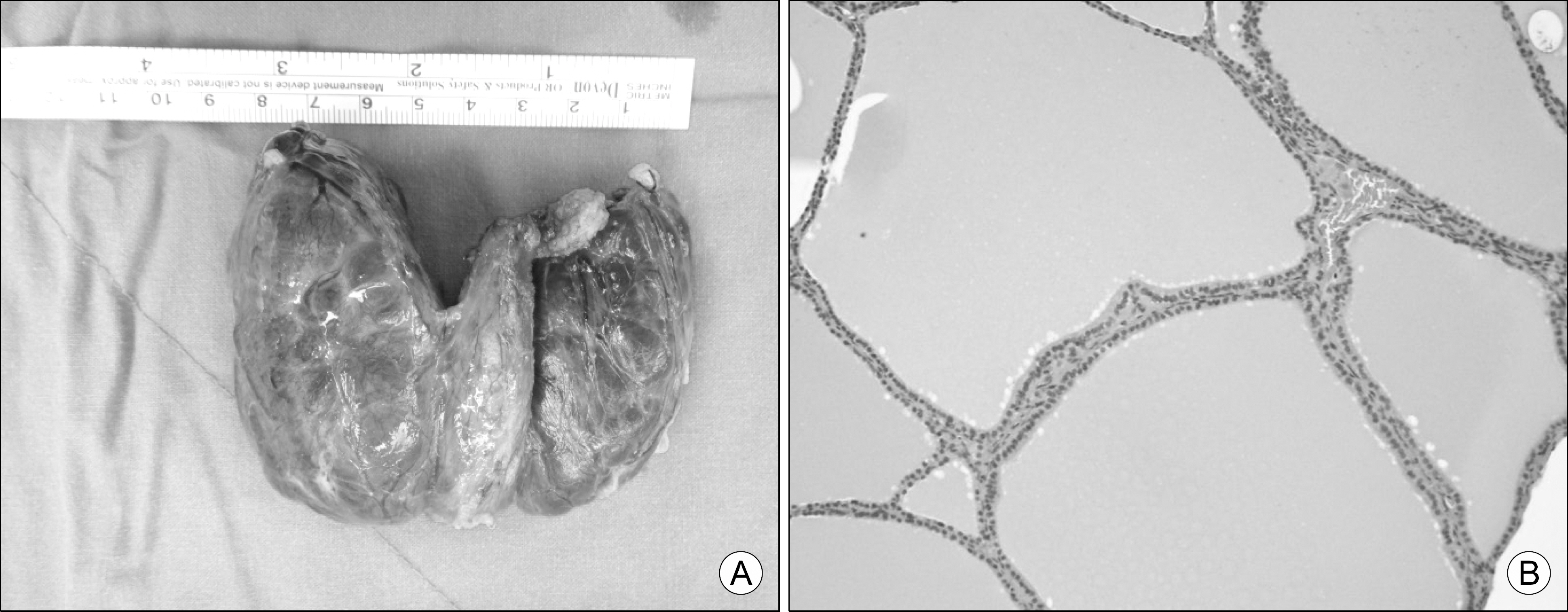
Fig. 3. Histopathologic images of the patients thyroid. (A) The postoperative gross image of the patients thyroid gland. Right lobe (7.0×4.0×3.5 cm), left lobe (5.0×5.0×3.0 cm), isthmus (3.0×2.0×1.0 cm) and pyramidal lobe, weighed 78 g in total. (B) Usually histologic findings of the Graves' disease are hyperplastic, and dilated follicles of variable sizes with scalloping of the colloid, but this case showed decreased scalloping of the colloid.
Reference
-
References
1. Ginsberg J. Diagnosis and management of Graves' disease. CMAJ. 2003; 168(5):575–85.2. Ma C, Xie J, Wang H, Li J, Chen S. Radioiodine therapy versus antithyroid medications for Graves' disease. Cochrane Database Syst Rev. 2016; 2:CD010094.
Article3. Pearce EN. Diagnosis and management of thyrotoxicosis. BMJ. 2006; 332(7554):1369–73.
Article4. Solomon BL, Wartofsky L, Burman KD. Adjunctive cholestyramine therapy for thyrotoxicosis. Clin Endocrinol (Oxf). 1993; 38(1):39–43.
Article5. Mercado M, Mendoza-Zubieta V, Bautista-Osorio R, Espinoza-de los Monteros AL. Treatment of hyperthyroidism with a combination of methimazole and cholestyramine. J Clin Endocrinol Metab. 1996; 81(9):3191–3.
Article6. Sebastian-Ochoa A, Quesada-Charneco M, Fernandez-Garcia D, Reyes-Garcia R, Rozas-Moreno P, Escobar-Jimenez F. Dramatic response to cholestyramine in a patient with Graves' disease resistant to conventional therapy. Thyroid. 2008; 18(10):1115–7.
Article7. Romaldini JH, Bromberg N, Werner RS, Tanaka LM, Rodrigues HF, Werner MC, et al. Comparison of effects of high and low dosage regimens of antithyroid drugs in the management of Graves' hyperthyroidism. J Clin Endocrinol Metab. 1983; 57(3):563–70.
Article8. Tomaski SM, Mahoney EM, Burgess LP, Raines KB, Bornemann M. Sodium ipodate (oragrafin) in the preoperative preparation of Graves' hyperthyroidism. Laryngoscope. 1997; 107(8):1066–70.
Article9. Tallstedt L, Lundell G, Torring O, Wallin G, Ljunggren JG, Blomgren H, et al. Occurrence of ophthalmopathy after treatment for Graves' hyperthyroidism. The Thyroid Study Group. N Engl J Med. 1992; 326(26):1733–8.10. Traisk F, Tallstedt L, Abraham-Nordling M, Andersson T, Berg G, Calissendorff J, et al. Thyroid-associated ophthalmopathy after treatment for Graves' hyperthyroidism with antithyroid drugs or iodine-131. J Clin Endocrinol Metab. 2009; 94(10):3700–7.11. Northcutt RC, Stiel JN, Hollifield JW, Stant EG Jr. The influence of cholestyramine on thyroxine absorption. JAMA. 1969; 208(10):1857–61.
Article12. Tsai WC, Pei D, Wang TF, Wu DA, Li JC, Wei CL, et al. The effect of combination therapy with propylthiouracil and cholestyramine in the treatment of Graves' hyperthyroidism. Clin Endocrinol (Oxf). 2005; 62(5):521–4.
Article13. Kaykhaei MA, Shams M, Sadegholvad A, Dabbaghmanesh MH, Omrani GR. Low doses of cholestyramine in the treatment of hyperthyroidism. Endocrine. 2008; 34(1–3):52–5.
Article14. Li H, Okuda J, Akamizu T, Mori T. A hyperthyroid patient with Graves' disease who was strongly resistant to methimazole: investigation on possible mechanisms of the resistance. Endocr J. 1995; 42(5):697–704.
Article15. Yang Y, Hwang S, Kim M, Lim Y, Kim MH, Lee S, et al. Refractory Graves' disease successfully cured by adjunctive cholestyramine and subsequent total thyroidectomy. Endocrinol Metab (Seoul). 2015; 30(4):620–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cholestyramine Use for Rapid Reversion to Euthyroid States in Patients with Thyrotoxicosis
- RE: Novel Application of Quantitative Single-Photon Emission Computed Tomography/Computed Tomography to Predict Early Response to Methimazole in Graves' Disease
- Refractory Graves' Disease Successfully Cured by Adjunctive Cholestyramine and Subsequent Total Thyroidectomy
- Ensulin Autoimmune Syndrome in a Patient with Methimazole-Treated Graves' Disease: A Case report
- A Case of Methimazole-induced Agranulocytosis and Kikuchi's Disease in a Patient with Graves' Disease
