Nerve-sparing techniques and results in robot-assisted radical prostatectomy
- Affiliations
-
- 1Department of Urology, Istanbul Bilim University, Istanbul, Turkey. hhtavukcu@yahoo.com
- KMID: 2361683
- DOI: http://doi.org/10.4111/icu.2016.57.S2.S172
Abstract
- Nerve-sparing techniques in robot-assisted radical prostatectomy (RARP) have advanced with the developments defining the prostate anatomy and robotic surgery in recent years. In this review we discussed the surgical anatomy, current nerve-sparing techniques and results of these operations. It is important to define the right and key anatomic landmarks for nerve-sparing in RARP which can demonstrate individual variations. The patients' risk assessment before the operation and intraoperative anatomic variations may affect the nerve-sparing technique, nerve-sparing degree and the approach. There is lack of randomized control trials for different nerve-sparing techniques and approaches in RARP, therefore accurate preoperative and intraoperative assessment of the patient is crucial. Current data shows that, performing the maximum possible nerve-sparing using athermal techniques have better functional outcomes.
MeSH Terms
Figure
-

Fig. 1 (A) Visceral component (yellow arrow) and parietal component (blue arrow) of the endopelvic fascia, arcus tendineus fascia pelvis (red dashed line). (B) Dissection of interfascial and intrafascial (nerve-sparing) plane. (C) Dissection of extrafascial plane, levator ani muscle (red arrow).
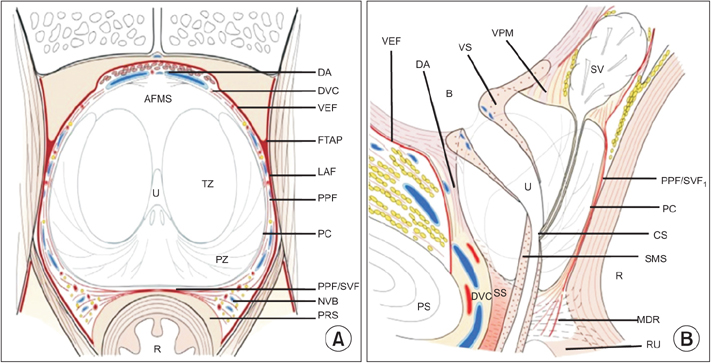
Fig. 2 (A) Axial section of prostatic and periprostatic fascia at midprostate. (B) Midline sagittal section of prostate, bladder and striated sphincter. AFMS, anterior fibromuscular stroma; B, bladder; CS, colliculus seminalis (verumontanum); DA, detrusor apron; DVC, dorsal vascular complex; FTAP, fascial tendineus arch of pelvis; LAF, levator ani fascia; MDR, medial dorsal raphe; NVB, neurovascular bundle; PC, pseudocapsule of prostate; PPF, periprostatic fascia; PPF/SVF, posterior prostatic fascia/seminal vesical fascia; PRS, perirectal space; PS, pubic symphysis; PZ, peripheral zone; R, rectum; RU, rectourethralis muscle; SMS, smooth muscle sphincter; SS, striated sphincter; SV, seminal vesicle; TZ, transition zone; U, urethra; VEF, visceral endopelvic fascia; VPM, vesicoprostatic muscle; VS, vesical sphincter. Adapted from Walz et al. Eur Urol 2016;70:301-11, with permission of Elsevier B.V. [34].

Fig. 3 (A) Coronal section of prostate, sphincteric urethra, periprostatic fascias and associated musculature. (B) Axial section through base of seminal vesicles to neurovascular bundle (NVB). B, bladder; M, midprostate; A, apex; U, urethra; CS, colliculus seminalis; CZ, central zone; LAF, levator ani fascia; PPF, periprostatic fascia; PC, pseudocapsule of prostate; ED, ejaculatory duct; LA, levator ani muscle; PF, prostatic fascia; PP, pelvic plexus; PPF/SVF, posterior prostatic fascia/ seminal vesicle fascia (Denonvilliers fascia); PZ, peripheral zone; R, rectum; SMS, smooth muscle sphincter; SS, striated sphincter; SV, seminal vesicle; VD, vas deferens; VPM, vesicoprostatic muscle. Adapted from Walz et al. Eur Urol 2010;57:179-92, with permission of Elsevier B.V. [17].
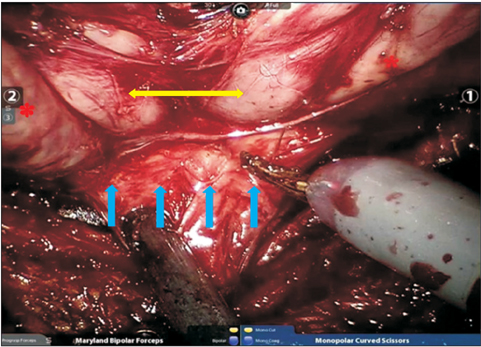
Fig. 4 Posterior prostatic dissection plane. Yellow arrow means vas deferens; blue arrows mean Denonvillier fascia; asterisk means seminal vesicles.
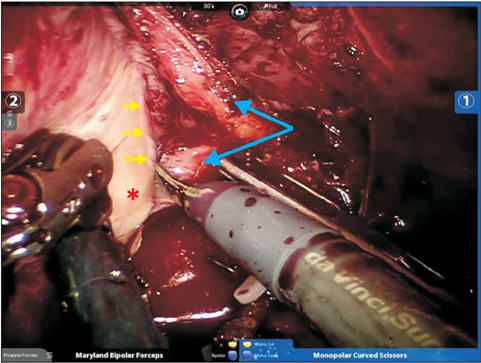
Fig. 5 Right intrafascial dissection; prostate and right neurovascular bundle (NVB). Yellow arrows mean dissection plane; blue arrow means NVB; asterisk means prostate capsule.
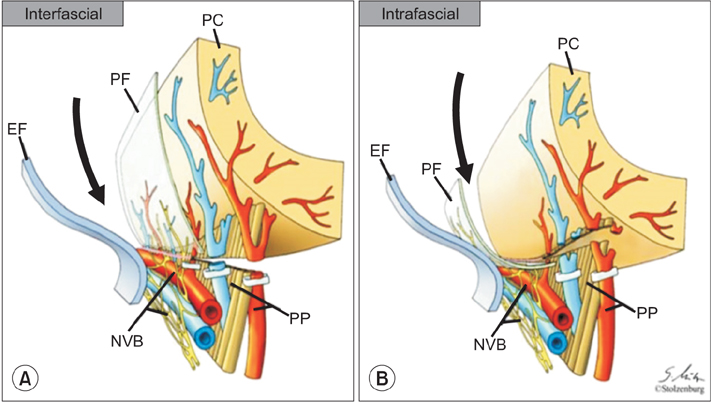
Fig. 6 Schematic drawing of 2 different surgical techniques for nerve-sparing prostatectomy. (A) Interfascial nerve-sparing prostatectomy. (B) Intrafascial nerve-sparing prostatectomy. EF, endopelvic fascia; PF, periprostatic fascia; PC, prostatic capsula; PP, prostatic pedicle; NBV, neurovascular bundle. Adapted from Stolzenburg et al. Eur Urol 2007:51:629-39, with permission of Elsevier B.V. [39].

Fig. 7 (A) Three dissection planes according to the Pasadena consensus [45], (B) Four dissection planes according to Tewari et al. [45], 1, dissection below veins, 2, dissection on the veins, 3, dissection distant from the veins, 4, extrafascial dissection, (C) Five dissection planes according to Schatloff et al. [55]: 1, extrafascial dissection; 2, sharp dissection distant from arteries; 3, sharp dissection on arteries; 4, sharp dissection on the level of arteries; 5, blunt dissection below arteries. Adapted from Walz et al. Eur Urol 2016;70:301-11, with permission of Elsevier B.V. [34].
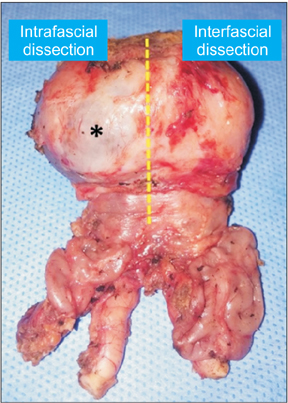
Fig. 8 View of prostate specimen, intrafascial dissection on right side, interfascial dissection on left side. Asterisk means prostate capsule; yellow line means posterior midline.

Fig. 9 (A) Antegrade neurovascular bundle (NVB) dissection on right side, (B) retrograde NVB dissection on left side. Yellow star means prostatic pedicle; blue arrow means prostate capsule; red dashed line and arrow mean NVB.
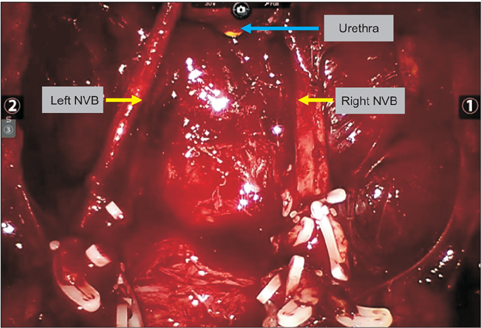
Fig. 10 Bilateral neurovascular bundle (NVB) after prostatectomy.
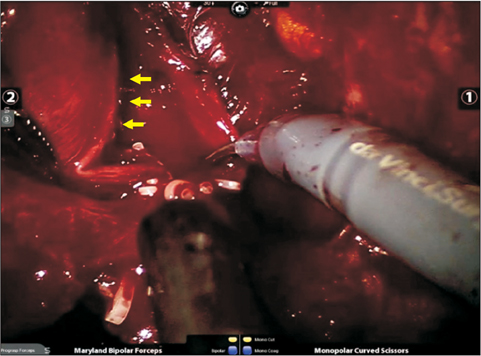
Fig. 11 Right landmark artery on right intrafascial dissection. Yellow arrows mean right landmark artery.
Cited by 1 articles
-
Lessons learned from 12,000 robotic radical prostatectomies: Is the journey as important as the outcome?
Sung Gu Kang, Ji Sung Shim, Fikret Onol, K. R. Seetharam Bhat, Vipul R. Patel
Investig Clin Urol. 2020;61(1):1-10. doi: 10.4111/icu.2020.61.1.1.
Reference
-
1. Edwards BK, Noone AM, Mariotto AB, Simard EP, Boscoe FP, Henley SJ, et al. Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer. 2014; 120:1290–1314.2. Ficarra V, Borghesi M, Suardi N, De Naeyer G, Novara G, Schatteman P, et al. Long-term evaluation of survival, continence and potency (SCP) outcomes after robot-assisted radical prostatectomy (RARP). BJU Int. 2013; 112:338–345.3. Ficarra V, Novara G, Artibani W, Cestari A, Galfano A, Graefen M, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol. 2009; 55:1037–1063.4. Coelho RF, Rocco B, Patel MB, Orvieto MA, Chauhan S, Ficarra V, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a critical review of outcomes reported by high-volume centers. J Endourol. 2010; 24:2003–2015.5. Willis DL, Gonzalgo ML, Brotzman M, Feng Z, Trock B, Su LM. Comparison of outcomes between pure laparoscopic vs robot-assisted laparoscopic radical prostatectomy: a study of comparative effectiveness based upon validated quality of life outcomes. BJU Int. 2012; 109:898–905.6. Asimakopoulos AD, Miano R, Di Lorenzo N, Spera E, Vespasiani G, Mugnier C. Laparoscopic versus robot-assisted bilateral nerve-sparing radical prostatectomy: comparison of pentafecta rates for a single surgeon. Surg Endosc. 2013; 27:4297–4304.7. Berge V, Berg RE, Hoff JR, Wessel N, Diep LM, Karlsen SJ, et al. A prospective study of transition from laparoscopic to robot-assisted radical prostatectomy: quality of life outcomes after 36-month follow-up. Urology. 2013; 81:781–786.8. Porpiglia F, Morra I, Lucci Chiarissi M, Manfredi M, Mele F, Grande S, et al. Randomised controlled trial comparing laparoscopic and robot-assisted radical prostatectomy. Eur Urol. 2013; 63:606–614.9. Asimakopoulos AD, Pereira Fraga CT, Annino F, Pasqualetti P, Calado AA, Mugnier C. Randomized comparison between laparoscopic and robot-assisted nerve-sparing radical prostatectomy. J Sex Med. 2011; 8:1503–1512.10. Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol. 1982; 128:492–497.11. Takenaka A, Hara R, Soga H, Murakami G, Fujisawa M. A novel technique for approaching the endopelvic fascia in retropubic radical prostatectomy, based on an anatomical study of fixed and fresh cadavers. BJU Int. 2005; 95:766–771.12. Savera AT, Kaul S, Badani K, Stark AT, Shah NL, Menon M. Robotic radical prostatectomy with the "Veil of Aphrodite" technique: histologic evidence of enhanced nerve sparing. Eur Urol. 2006; 49:1065–1073.13. Ayala AG, Ro JY, Babaian R, Troncoso P, Grignon DJ. The prostatic capsule: does it exist? Its importance in the staging and treatment of prostatic carcinoma. Am J Surg Pathol. 1989; 13:21–27.14. Myers RP, Villers A. Anatomic considerations in radical prostatectomy. In : Kirby RS, Partin AW, Feneley M, Parsons JK, editors. Prostate cancer: principles and practice. London: Taylor & Francis;2006. p. 701–713.15. Stolzenburg JU, Rabenalt R, Do M, Schwalenberg T, Winkler M, Dietel A, et al. Intrafascial nerve-sparing endoscopic extraperitoneal radical prostatectomy. Eur Urol. 2008; 53:931–940.16. Tewari AK, Bigelow K, Rao S, Takenaka A, El-Tabi N, Te A, et al. Anatomic restoration technique of continence mechanism and preservation of puboprostatic collar: a novel modification to achieve early urinary continence in men undergoing robotic prostatectomy. Urology. 2007; 69:726–731.17. Walz J, Burnett AL, Costello AJ, Eastham JA, Graefen M, Guillonneau B, et al. A critical analysis of the current knowledge of surgical anatomy related to optimization of cancer control and preservation of continence and erection in candidates for radical prostatectomy. Eur Urol. 2010; 57:179–192.18. Menon M, Shrivastava A, Kaul S, Badani KK, Fumo M, Bhandari M, et al. Vattikuti Institute prostatectomy: contemporary technique and analysis of results. Eur Urol. 2007; 51:648–657.19. Nielsen ME, Schaeffer EM, Marschke P, Walsh PC. High anterior release of the levator fascia improves sexual function following open radical retropubic prostatectomy. J Urol. 2008; 180:2557–2564.20. Kourambas J, Angus DG, Hosking P, Chou ST. A histological study of Denonvilliers' fascia and its relationship to the neurovascular bundle. Br J Urol. 1998; 82:408–410.21. Costello AJ, Brooks M, Cole OJ. Anatomical studies of the neurovascular bundle and cavernosal nerves. BJU Int. 2004; 94:1071–1076.22. Kiyoshima K, Yokomizo A, Yoshida T, Tomita K, Yonemasu H, Nakamura M, et al. Anatomical features of periprostatic tissue and its surroundings: a histological analysis of 79 radical retropubic prostatectomy specimens. Jpn J Clin Oncol. 2004; 34:463–468.23. Lindsey I, Guy RJ, Warren BF, Mortensen NJ. Anatomy of Denonvilliers' fascia and pelvic nerves, impotence, and implications for the colorectal surgeon. Br J Surg. 2000; 87:1288–1299.24. Villers A, McNeal JE, Freiha FS, Boccon-Gibod L, Stamey TA. Invasion of Denonvilliers' fascia in radical prostatectomy specimens. J Urol. 1993; 149:793–798.25. van Ophoven A, Roth S. The anatomy and embryological origins of the fascia of Denonvilliers: a medico-historical debate. J Urol. 1997; 157:3–9.26. Lepor H, Gregerman M, Crosby R, Mostofi FK, Walsh PC. Precise localization of the autonomic nerves from the pelvic plexus to the corpora cavernosa: a detailed anatomical study of the adult male pelvis. J Urol. 1985; 133:207–212.27. Lunacek A, Schwentner C, Fritsch H, Bartsch G, Strasser H. Anatomical radical retropubic prostatectomy: 'curtain dissection' of the neurovascular bundle. BJU Int. 2005; 95:1226–1231.28. Epstein JI. Pathologic assessment of the surgical specimen. Urol Clin North Am. 2001; 28:567–594.29. Quinlan DM, Epstein JI, Carter BS, Walsh PC. Sexual function following radical prostatectomy: influence of preservation of neurovascular bundles. J Urol. 1991; 145:998–1002.30. Tewari A, Takenaka A, Mtui E, Horninger W, Peschel R, Bartsch G, et al. The proximal neurovascular plate and the tri-zonal neural architecture around the prostate gland: importance in the athermal robotic technique of nerve-sparing prostatectomy. BJU Int. 2006; 98:314–323.31. Ganzer R, Blana A, Gaumann A, Stolzenburg JU, Rabenalt R, Bach T, et al. Topographical anatomy of periprostatic and capsular nerves: quantification and computerised planimetry. Eur Urol. 2008; 54:353–360.32. Alsaid B, Bessede T, Diallo D, Moszkowicz D, Karam I, Benoit G, et al. Division of autonomic nerves within the neurovascular bundles distally into corpora cavernosa and corpus spongiosum components: immunohistochemical confirmation with three-dimensional reconstruction. Eur Urol. 2011; 59:902–909.33. Clarebrough EE, Challacombe BJ, Briggs C, Namdarian B, Weston R, Murphy DG, et al. Cadaveric analysis of periprostatic nerve distribution: an anatomical basis for high anterior release during radical prostatectomy? J Urol. 2011; 185:1519–1525.34. Walz J, Epstein JI, Ganzer R, Graefen M, Guazzoni G, Kaouk J, et al. A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: An Update. Eur Urol. 2016; 70:301–311.35. Potdevin L, Ercolani M, Jeong J, Kim IY. Functional and oncologic outcomes comparing interfascial and intrafascial nerve sparing in robot-assisted laparoscopic radical prostatectomies. J Endourol. 2009; 23:1479–1484.36. Shikanov S, Woo J, Al-Ahmadie H, Katz MH, Zagaja GP, Shalhav AL, et al. Extrafascial versus interfascial nerve-sparing technique for robotic-assisted laparoscopic prostatectomy: comparison of functional outcomes and positive surgical margins characteristics. Urology. 2009; 74:611–616.37. Martinez-Salamanca JI, Ramanathan R, Rao S, Mandhani A, Leung R, Horninger W, et al. Second Prize: Pelvic neuroanatomy and innovative approaches to minimize nerve damage and maximize cancer control in patients undergoing robot-assisted radical prostatectomy. J Endourol. 2008; 22:1137–1146.38. Carter S, Le JD, Hu JC. Anatomic and technical considerations for optimizing recovery of sexual function during robotic-assisted radical prostatectomy. Curr Opin Urol. 2013; 23:88–94.39. Stolzenburg JU, Schwalenberg T, Horn LC, Neuhaus J, Constantinides C, Liatsikos EN. Anatomical landmarks of radical prostatecomy. Eur Urol. 2007; 51:629–639.40. Montorsi F, Wilson TG, Rosen RC, Ahlering TE, Artibani W, Carroll PR, et al. Best practices in robot-assisted radical prostatectomy: recommendations of the Pasadena Consensus Panel. Eur Urol. 2012; 62:368–381.41. Alemozaffar M, Duclos A, Hevelone ND, Lipsitz SR, Borza T, Yu HY, et al. Technical refinement and learning curve for attenuating neurapraxia during robotic-assisted radical prostatectomy to improve sexual function. Eur Urol. 2012; 61:1222–1228.42. Patel VR, Coelho RF, Chauhan S, Orvieto MA, Palmer KJ, Rocco B, et al. Continence, potency and oncological outcomes after robotic-assisted radical prostatectomy: early trifecta results of a high-volume surgeon. BJU Int. 2010; 106:696–702.43. Menon M, Shrivastava A, Bhandari M, Satyanarayana R, Siva S, Agarwal PK. Vattikuti Institute prostatectomy: technical modifications in 2009. Eur Urol. 2009; 56:89–96.44. Kumar A, Tandon S, Samavedi S, Mouraviev V, Bates AS, Patel VR. Current status of various neurovascular bundle-sparing techniques in robot-assisted radical prostatectomy. J Robot Surg. 2016; 10:187–200.45. Tewari AK, Srivastava A, Huang MW, Robinson BD, Shevchuk MM, Durand M, et al. Anatomical grades of nerve sparing: a risk-stratified approach to neural-hammock sparing during robot-assisted radical prostatectomy (RARP). BJU Int. 2011; 108(6 Pt 2):984–992.46. Inoue S, Shiina H, Hiraoka T, Mitsui Y, Sumura M, Urakami S, et al. Retrospective analysis of the distance between the neurovascular bundle and prostate cancer foci in radical prostatectomy specimens: its clinical implication in nerve-sparing surgery. BJU Int. 2009; 104:1085–1090.47. Ko YH, Coelho RF, Sivaraman A, Schatloff O, Chauhan S, Abdul-Muhsin HM, et al. Retrograde versus antegrade nerve sparing during robot-assisted radical prostatectomy: which is better for achieving early functional recovery? Eur Urol. 2013; 63:169–177.48. Kaul S, Savera A, Badani K, Fumo M, Bhandari A, Menon M. Functional outcomes and oncological efficacy of Vattikuti Institute prostatectomy with Veil of Aphrodite nerve-sparing: an analysis of 154 consecutive patients. BJU Int. 2006; 97:467–472.49. Chien GW, Mikhail AA, Orvieto MA, Zagaja GP, Sokoloff MH, Brendler CB, et al. Modified clipless antegrade nerve preservation in robotic-assisted laparoscopic radical prostatectomy with validated sexual function evaluation. Urology. 2005; 66:419–423.50. Badani KK, Shapiro EY, Berg WT, Kaufman S, Bergman A, Wambi C, et al. A pilot study of laparoscopic Doppler ultrasound probe to map arterial vascular flow within the neurovascular bundle during robot-assisted radical prostatectomy. Prostate Cancer. 2013; 2013:810715.51. Ahlering TE, Eichel L, Chou D, Skarecky DW. Feasibility study for robotic radical prostatectomy cautery-free neurovascular bundle preservation. Urology. 2005; 65:994–997.52. Finley DS, Osann K, Skarecky D, Ahlering TE. Hypothermic nerve-sparing radical prostatectomy: rationale, feasibility, and effect on early continence. Urology. 2009; 73:691–696.53. Patel VR, Samavedi S, Bates AS, Kumar A, Coelho R, Rocco B, et al. Dehydrated human amnion/chorion membrane allograft nerve wrap around the prostatic neurovascular bundle accelerates early return to continence and potency following robot-assisted radical prostatectomy: propensity score-matched analysis. Eur Urol. 2015; 67:977–980.54. Srivastava A, Chopra S, Pham A, Sooriakumaran P, Durand M, Chughtai B, et al. Effect of a risk-stratified grade of nerve-sparing technique on early return of continence after robot-assisted laparoscopic radical prostatectomy. Eur Urol. 2013; 63:438–444.55. Schatloff O, Chauhan S, Sivaraman A, Kameh D, Palmer KJ, Patel VR. Anatomic grading of nerve sparing during robotassisted radical prostatectomy. Eur Urol. 2012; 61:796–802.56. Patel VR, Schatloff O, Chauhan S, Sivaraman A, Valero R, Coelho RF, et al. The role of the prostatic vasculature as a landmark for nerve sparing during robot-assisted radical prostatectomy. Eur Urol. 2012; 61:571–576.57. Finley DS, Rodriguez E Jr, Skarecky DW, Ahlering TE. Quantitative and qualitative analysis of the recovery of potency after radical prostatectomy: effect of unilateral vs bilateral nerve sparing. BJU Int. 2009; 104:1484–1489.58. Greco F, Hoda MR, Wagner S, Reichelt O, Inferrera A, Magno C, et al. Bilateral vs unilateral laparoscopic intrafascial nerve-sparing radical prostatectomy: evaluation of surgical and functional outcomes in 457 patients. BJU Int. 2011; 108:583–587.59. Ficarra V, Novara G, Fracalanza S, D'Elia C, Secco S, Iafrate M, et al. A prospective, non-randomized trial comparing robot-assisted laparoscopic and retropubic radical prostatectomy in one European institution. BJU Int. 2009; 104:534–539.60. Rocco B, Matei DV, Melegari S, Ospina JC, Mazzoleni F, Errico G, et al. Robotic vs open prostatectomy in a laparoscopically naive centre: a matched-pair analysis. BJU Int. 2009; 104:991–995.61. Krambeck AE, DiMarco DS, Rangel LJ, Bergstralh EJ, Myers RP, Blute ML, et al. Radical prostatectomy for prostatic adenocarcinoma: a matched comparison of open retropubic and robot-assisted techniques. BJU Int. 2009; 103:448–453.62. Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, et al. Pentafecta: a new concept for reporting outcomes of robot-assisted laparoscopic radical prostatectomy. Eur Urol. 2011; 59:702–707.63. Kowalczyk KJ, Huang AC, Hevelone ND, Lipsitz SR, Yu HY, Ulmer WD, et al. Stepwise approach for nerve sparing without countertraction during robot-assisted radical prostatectomy: technique and outcomes. Eur Urol. 2011; 60:536–547.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial experience with Retzius-sparing robot-assisted radical prostatectomy compared to the conventional method: is it a suitable option for robotic prostatectomy beginners?
- Erratum: Robot-Assisted Laparoscopic Radical Prostatectomy
- Simultaneous Robot-Assisted Laparoendoscopic Single-Site Partial Nephrectomy and Standard Radical Prostatectomy
- Simultaneous Retzius-sparing robot-assisted radical prostatectomy and partial nephrectomy
- A Case of Robot-Assisted Laparoscopic Radical Prostatectomy in Primary Small Cell Prostate Cancer
