J Korean Ophthalmol Soc.
2016 Nov;57(11):1752-1758. 10.3341/jkos.2016.57.11.1752.
Surgical Outcomes Dependent on the Amount of Hyperopia in Infantile Esotropia
- Affiliations
-
- 1Department of Ophthalmology, Gachon University Gil Hospital, Incheon, Korea. hjpaik@gilhospital.com
- KMID: 2357731
- DOI: http://doi.org/10.3341/jkos.2016.57.11.1752
Abstract
- PURPOSE
In the present study, short-term and long-term surgical outcomes dependent on the amount of hyperopia in patients with infantile esotropia were analyzed.
METHODS
In this study, 80 patients with infantile esotropia who underwent both medial rectus recession from 2007 to 2011 and followed up for at least 36 months were retrospectively examined. The patients were divided into two groups according to the degree of hyperopia: ≥ +3.0 D (high hyperopia [HH], n = 59 patients) and < +3.0 D (non-high hyperopia [NH], n = 21 patients). Clinical characteristics analyzed included surgical success rate and dose-response relationship at the 3-month and 3-year postoperative follow-ups.
RESULTS
Initial preoperative alignment (NH: 44.8 ± 10.2 PD, HH: 42.7 ± 11.6 PD, p = 0.450), surgical success rates (NH: 69.5% (41/59), HH: 71.4% (15/21), p = 0.837), under-correction rates (NH: 23.7% (14/59), HH: 9.5% (2/21), p = 0.191) and over-correction rates (NH: 6.8% (4/59), HH: 19.1% (4/21), p = 0.138) were not statistically significantly different between the NH and HH groups. A tendency towards a larger dose-response relationship was observed with HH (NH: 3.9 PD/mm, HH: 4.3 PD/mm) at the 3-month postoperative follow-up, but was not significant (p = 0.105). At the 3-year postoperative follow-up, exodrift was in progress and the dose-response relationship was significantly higher in the HH group than NH group (NH: 3.9 PD/mm, HH: 4.9 PD/mm, p = 0.010). A difference between the groups with amblyopia was observed (NH: 8.5% (5/59), HH: 23.8% (5/21), p = 0.146), although without statistical significance.
CONCLUSIONS
The surgical success rate of infantile esotropia was not statistically associated with the amount of hyperopia. There was no statistical association between the dose-response relationship and amount of hyperopia at the postoperative 3-month follow-up, but a statistical association was found in the high dose-response relationship in the HH group at the postoperative 3-year follow-up. Therefore, the conventional amount of recession or muscle resection should be modified in high hyperopic (≥ +3.0 D) infantile esotropia, and long-term postoperative follow-up is necessary.
Keyword
MeSH Terms
Figure
-
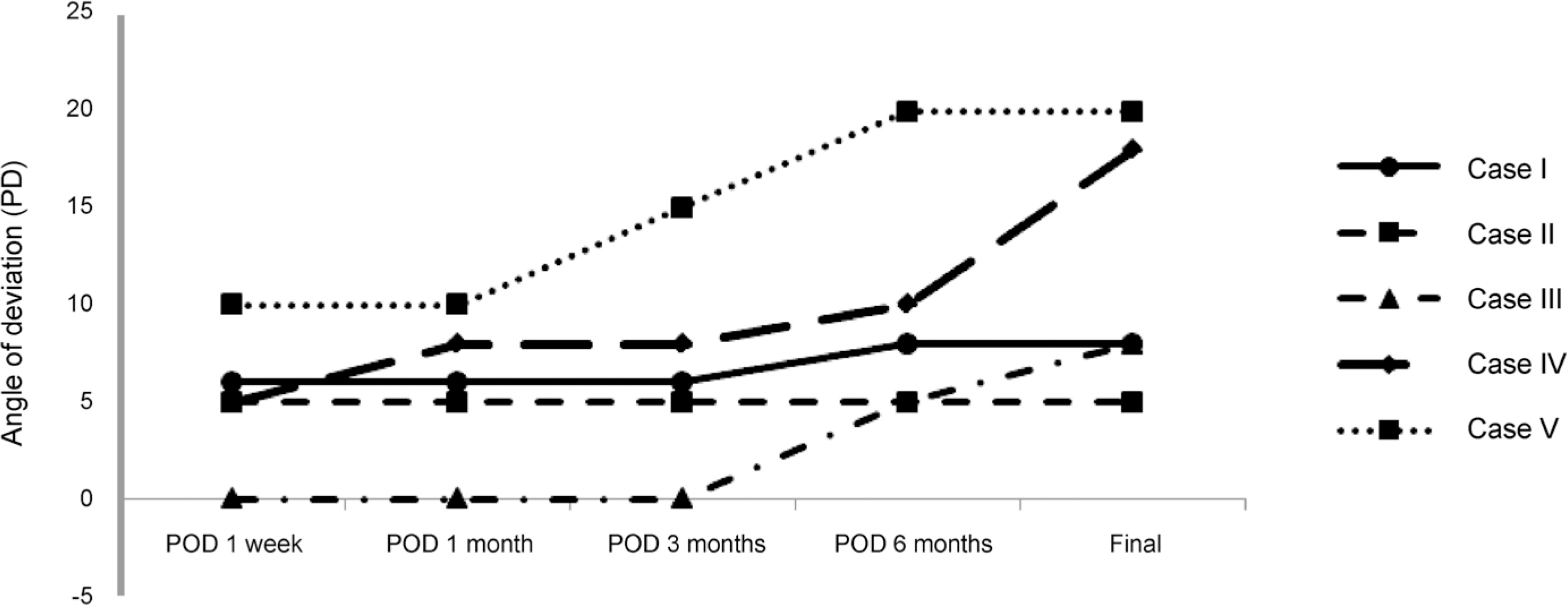
Figure 1. Post-op angle of deviation – patients with refractive error ≥+5.0 D. Post-op exodrift was more in patients with refractive error ≥+5.0 D. PD = prism diopters; POD = post-op day.
Reference
-
References
1. Ing M, Costenbader FD, Parks MM, Albert DG. Early surgery for congenital esotropia. Am J Ophthalmol. 1966; 61:1419–27.
Article2. Helvestone EM. 19th annual Frank Costenbader Lecture–The abdominal of congenital esotropia. J Pediatr Ophthalmol Strabismus. 1933; 30:215–32.3. Zubcov AA, Reinecke RD, Calhoun JH. Asymmetric horizontal tropias, DVD, and manifest latent nystagmus: an explanation of dissociated horizontal deviation. J Pediatr Ophthalmol Strabismus. 1990; 27:59–64. discussion 65.4. Wilson ME, McClatchey SK. Dissociated horizontal deviation. J Pediatr Ophthalmol Strabismus. 1991; 28:90–5.
Article5. Parks MM. Symposium: infantile esotorpia. Summary and conclusions. Am J Orthopt J. 1968; 18:19–22.6. Fisher NF, Flom MC, Jampolsky A. Early surgery of congenital esotropia. Am J Ophthalmol. 1968; 65:439–43.
Article7. Von Noorden GK, Isaza A, Parks ME. Surgical treatment of abdominal esotropia. Trans Am Acad Ophthalmol Otolaryngol. 1972; 76:1465–78.8. Kraft SP, Scott WE. Surgery for congenital esotropia–An Age Comparison Study. J Pediatr Ophthalmol Strabismus. 1984; 21:57–68.9. Kushner BJ, Fisher MR, Lucchese NJ, Morton GV. Factors abdominal response to strabismus surgery. Arch Ophthalmol. 1993; 111:75–9.10. Mims JL III, Treff G, Kincaid M, et al. Quantitative surgical abdominal for bimedial recession for infantile esotropia. Binocul Vis Strabismus. 1985; 1:7–22.11. Pickering JD, Simon JW, Lininger LL, et al. Exaggerated effect of bilateral medial rectus recession in developmentally delayed children. J Pediatr Ophthalmol Strabismus. 1994; 31:374–7.
Article12. Kushner BJ, Morton GV. The effect of surgical technique and amount, patient age, abduction quality and deviation magnitude on surgical success rates in infantile esotropia. Binocular Vis Strabismus. 1987; 2:25–40.13. Ingram RM. Refraction as a basis for screening children for squint and amblyopia. Br J Ophthalmol. 1977; 61:8–15.
Article14. Khan AO. The relationships among cycloplegic refraction, abdominal, and axial length in children with refractive abdominal esotropia. J AAPOS. 2011; 15:241–4.15. Shauly Y, Miller B, Meyer E. Clinical characteristics and long-term postoperative results of infantile esotropia and myopia. J Pediatr Ophthalmol Strabismus. 1997; 34:357–64.
Article16. Mohney BG. Common forms of childhood esotropia. Ophthalmology. 2001; 108:805–9.
Article17. Wright KW. Esodeviations. Wright KW, Spiegle PH, editors. Pediatric Ophthalmology and Strabismus. 2nd ed.New York: Springer;2003. chap. 13.
Article18. Kim C, Hwang JM. The clinical course of esotropia associated with hypermetropia after initial wearing of glasses. J Korean Ophthalmol Soc. 2003; 44:134–43.19. Von Noorden GK. Binocular Vision and Ocular Motility. 6th ed.St. Louis: Mosby;2002. p. 313.20. Atkinson J, Braddick O, Robier B, et al. Two infant vision screening programmes: prediction and prevention of strabismus and abdominal from photo- and videorefractive screening. Eye (Lond). 1996; 10(Pt 2):189–98.21. Noh JH, Kim SY. Comparison of clinical features in hypermetropic children according to refractive error. J Korean Ophthalmol Soc. 2015; 56:1416–23.
Article22. Kim IN, Paik HJ. abdominal changes of hyperopic refractive error in refractive accommodative esotropia. J Korean Ophthalmol Soc. 2015; 56:580–5.23. Jun JH, Lee YC, Lee SY. Clinical features of refractive abdominal esotropia according to degree of hypermetropia. J Korean Ophthalmol Soc. 2008; 49:617–22.24. Parks MM. Abnormal accommodative convergence in squint. AMA Arch Ophthalmol. 1958; 59:364–80.
Article25. Yang H, Chang YH, Lee JB. Clinical features of refractive abdominal esotropia and partially accommodative esotropia. J Korean Ophthalmol Soc. 2004; 45:626–30.26. Choi KS, Chang JH, Chang YH, Lee JB. Occurrence and risk abdominals of decompensation and additional treatment in refractive abdominal esotropia. J Korean Ophthalmol Soc. 2006; 47:121–6.27. Kim HK, Chung HJ, Park SH, Shin SY. Consecutive exotropia abdominal bilateral medial rectus recession for infantile esotropia. J Korean Ophthalmol Soc. 2009; 50:1712–16.28. Magli A, Carelli R, Matarazzo F, Bruzzese D. Essential infantile esotropia: postoperative motor outcomes and inferential analysis of strabismus surgery. BMC Ophthalmol. 2014; 14:35.
Article29. Spierer O, Spierer A. Comparison of hang-back and conventional bimedial rectus recession in infantile esotropia. Graefes Arch Clin Exp Ophthalmol. 2010; 248:901–5.
Article30. Lee JR, Roh YB. The Factors affecting consecutive exotropia with angel of 20 prism diopters or more following surgery for esotropia. J Korean Ophthalmol Soc. 1995; 36:1778–83.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Clinical Features in Hypermetropic Children According to Refractive Error
- Five-Year Follow-up Results of Refractive Accommodative Esotropia
- Surgical Outcome of Esotropia Considering the Functional Equator
- Spontaneous Consecutive Exotropia
- Clinical Features of Refractive Accommodative Esotropia According to Degree of Hypermetropia
