Characteristics of Chest Lesions Missed on Neck CT Interpretations
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. ami@catholic.ac.kr
- KMID: 2355991
- DOI: http://doi.org/10.3348/jksr.2016.75.5.376
Abstract
- PURPOSE
The purpose of this study was to identify the characteristics of chest lesions that are missed in interpretations of neck computed tomography (CT) scans.
MATERIALS AND METHODS
A total of 240 consecutive neck CT scans were retrospectively analyzed to determine whether chest lesions were included or not. All missed chest lesions, which had not been described on neck CT reports, were recorded, and classified according to their clinical significance (insignificant, indeterminate, or significant) and awareness (known or unknown) at the time of CT interpretation, and their radiologic patterns were analyzed.
RESULTS
Eighty seven (36.3%) of 240 neck CT scans had 105 chest lesions, and 88 of these were not described on the neck CT reports. Thirty seven clinically known or insignificant lesions were excluded, resulting in a miss rate for chest lesions of 35.2% (37/105), with six of these (5.7%) being potentially significant. The most common location of missed chest lesions was the lung (56/88, 63.6%), and 45 (80.4%) of these missed lung lesions were visualized only with lung window settings.
CONCLUSION
Chest lesions were common and frequently missed on neck CT interpretations. When reviewing neck CT scans, a special attention should be given to lung lesions by using lung window settings.
Figure
-
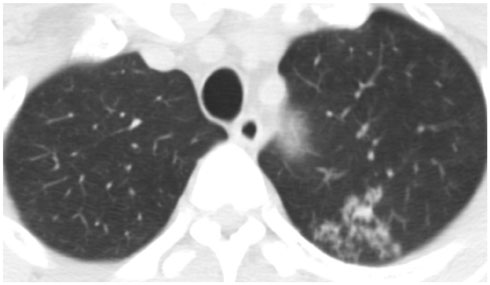
Fig. 1 Neck CT image at the level of lung apex in a 42-year-old man presenting with tongue discomfort. Multiple clustered, centrilobular nodules are noted in the left upper lobe, raising the possibility of pulmonary tuberculosis, which were missed on neck CT interpretation.

Fig. 2 Neck CT at the level of lung apex in a 53-year-old man with peritonsilar abscess. CT image with lung window setting shows multiple variable sized bullae in the right lung apex, which was not described in neck CT report. Minimal centrilobular emphysema is also noted in the left upper lobe.
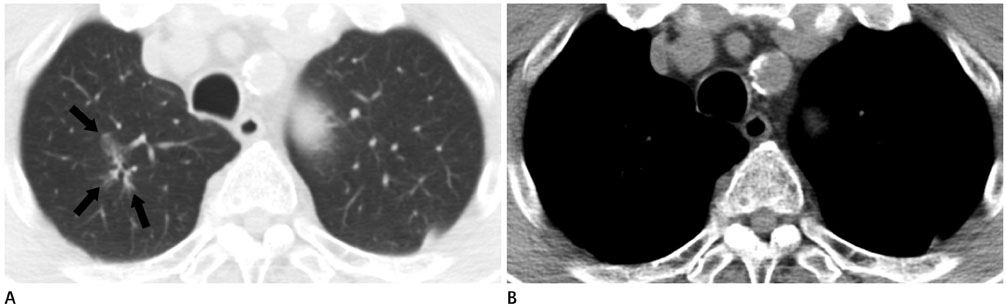
Fig. 3 Missed and significant chest lesion on neck CT in an 80-year-old man with thyroid cancer. The lower part of neck CT image with lung window setting (A) shows an irregular shaped peribronchial ground-glass opacity nodule (arrows) in the right upper lobe, suggesting adenocarcinoma of the lung. On mediastinal window setting (B), this lesion is not seen.
Reference
-
1. Briggs GM, Flynn PA, Worthington M, Rennie I, McKinstry CS. The role of specialist neuroradiology second opinion reporting: is there added value? Clin Radiol. 2008; 63:791–795.2. Donald JJ, Barnard SA. Common patterns in 558 diagnostic radiology errors. J Med Imaging Radiat Oncol. 2012; 56:173–178.3. Sosna J, Esses SJ, Yeframov N, Bernstine H, Sella T, Fraifeld S, et al. Blind spots at oncological CT: lessons learned from PET/CT. Cancer Imaging. 2012; 12:259–268.4. Katz DS, Jorgensen MJ, Rubin GD. Detection and follow-up of important extra-arterial lesions with helical CT angiography. Clin Radiol. 1999; 54:294–300.5. Koonce J, Schoepf JU, Nguyen SA, Northam MC, Ravenel JG. Extra-cardiac findings at cardiac CT: experience with 1,764 patients. Eur Radiol. 2009; 19:570–576.6. Yee J, Kumar NN, Godara S, Casamina JA, Hom R, Galdino G, et al. Extracolonic abnormalities discovered incidentally at CT colonography in a male population. Radiology. 2005; 236:519–526.7. Fitzgerald R. Error in radiology. Clin Radiol. 2001; 56:938–946.8. Pinto A, Brunese L, Pinto F, Reali R, Daniele S, Romano L. The concept of error and malpractice in radiology. Semin Ultrasound CT MR. 2012; 33:275–279.9. McCreadie G, Oliver TB. Eight CT lessons that we learned the hard way: an analysis of current patterns of radiological error and discrepancy with particular emphasis on CT. Clin Radiol. 2009; 64:491–499. discussion 500-501.10. Renfrew DL, Franken EA Jr, Berbaum KS, Weigelt FH, Abu-Yousef MM. Error in radiology: classification and lessons in 182 cases presented at a problem case conference. Radiology. 1992; 183:145–150.11. Robinson PJ. Radiology’s Achilles’ heel: error and variation in the interpretation of the Röntgen image. Br J Radiol. 1997; 70:1085–1098.12. Kim YW, Mansfield LT. Fool me twice: delayed diagnoses in radiology with emphasis on perpetuated errors. AJR Am J Roentgenol. 2014; 202:465–470.13. Lian K, Bharatha A, Aviv RI, Symons SP. Interpretation errors in CT angiography of the head and neck and the benefit of double reading. AJNR Am J Neuroradiol. 2011; 32:2132–2135.14. Strub WM, Leach JL, Tomsick T, Vagal A. Overnight preliminary head CT interpretations provided by residents: locations of misidentified intracranial hemorrhage. AJNR Am J Neuroradiol. 2007; 28:1679–1682.15. Alpert JB, Fantauzzi JP, Melamud K, Greenwood H, Naidich DP, Ko JP. Clinical significance of lung nodules reported on abdominal CT. AJR Am J Roentgenol. 2012; 198:793–799.16. de Bree R, Deurloo EE, Snow GB, Leemans CR. Screening for distant metastases in patients with head and neck cancer. Laryngoscope. 2000; 110(3 Pt 1):397–401.17. Albertyn LE. Extending the search pattern in computed tomography. Clin Radiol. 1987; 38:145–149.18. Siegle RL, Baram EM, Reuter SR, Clarke EA, Lancaster JL, McMahan CA. Rates of disagreement in imaging interpretation in a group of community hospitals. Acad Radiol. 1998; 5:148–154.19. Goddard P, Leslie A, Jones A, Wakeley C, Kabala J. Error in radiology. Br J Radiol. 2001; 74:949–951.20. Berlin L. Radiologic errors and malpractice: a blurry distinction. AJR Am J Roentgenol. 2007; 189:517–522.21. Borgstede JP, Lewis RS, Bhargavan M, Sunshine JH. RADPEER quality assurance program: a multifacility study of interpretive disagreement rates. J Am Coll Radiol. 2004; 1:59–65.22. Arendts G, Manovel A, Chai A. Cranial CT interpretation by senior emergency department staff. Australas Radiol. 2003; 47:368–374.23. Kim ES, Yoon DY, Lee HY, Ku YJ, Han A, Yoon SJ, et al. Comparison of emergency cranial CT interpretation between radiology residents and neuroradiologists: transverse versus three-dimensional images. Diagn Interv Radiol. 2014; 20:277–284.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnostic Usefulness of Routinely Performed Preoperative Chest Computed Tomography for Colorectal Cancer
- Evaluation of the Accuracy of Abdominal Ultrasound Focusing on the Missed Lesions Based on the Abdominal Computed Tomography in Health Screening
- Radiologic Findings of Thoracic Inlet Lesions
- Characteristics of Missed Simultaneous Gastric Lesions Based on Double-Check Analysis of the Endoscopic Image
- Evaluation of the Significance of Incidental Breast Lesions Detected by Chest CT
