Extraction of a Fully Deployed Coronary Stent during Retrieval of Another Dislodged Stent
- Affiliations
-
- 1Cardiovascular Center, Pusan National University Yangsan Hospital, Division of Cardiology, Department of Internal Medicine, Pusan National University School of Medicine, Yangsan, Korea. ptca82@gmail.com
- KMID: 2355464
- DOI: http://doi.org/10.4070/kcj.2016.46.6.862
Abstract
- Coronary stent dislodgement is a rare and serious complication of percutaneous coronary intervention and is associated with major adverse cardiac events. Successful retrieval of the stent is recommended in this situation because it is important for the prognosis. Recently, a patient was referred to our hospital with a dislodged coronary stent. When attempting to percutaneously extract the dislodged stent, a challenging situation was encountered, as the stent was entrapped and tightly entangled with another fully deployed coronary stent. Extraction of a fully deployed stent is generally prohibited as it may result in severe complications. Nevertheless, we extracted both the dislodged stent and the fully deployed stent, as a last resort. Herein, we report about this case. Our case highlights if the operator had a thorough understanding of the surrounding circumstances regarding the fully deployed coronary stent, successful extraction of the fully deployed coronary stent without any complications could be possible.
Figure
-

Fig. 1 Baseline coronary angiogram. (A) Left anterior oblique cranial view shows a diffused long lesion with a very small right coronary artery (RCA). (B) Two stents were inserted at the proximal and mid segments of the RCA.

Fig. 2 Fluoroscopic images of the procedure. (A) The operator at the local hospital failed to deliver a second stent into the distal RCA. While attempting to retract the undeployed stent (white arrow) into the guiding catheter, the stent was entrapped by the fully deployed stent in the proximal RCA (white arrow head) and totally detached from the stent balloon. (B) We were able to capture the middle portion of the undeployed dislodged stent (white arrow) using a multi-snare catheter. (C) Under manual retraction, the proximal RCA deployed stent (white arrow head) was elongated but not detached from the undeployed dislodged stent (white arrow). (D) Under continuous retraction, the captured undeployed stent (white arrow) was bent in half and successfully retrieved into the guiding catheter. (G) Finally, both the maximally elongated proximal RCA stent (white arrow head) and the bent, partially dislodged stent (white arrow) were successfully retrieved into the guiding catheter. (H) Final CAG of the RCA showed excellent results with TIMI grade 3 distal flow. RCA: right coronary artery, CAG: coronary angiogram, TIMI: thrombolysis in myocardial infarction.
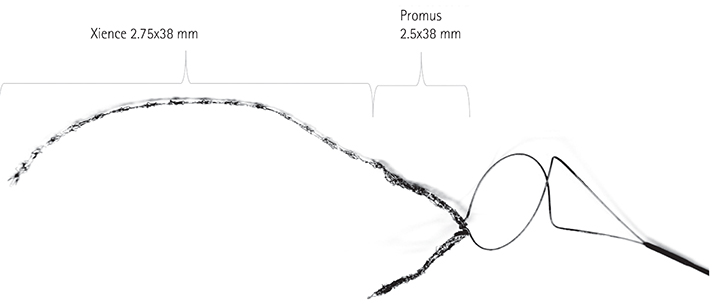
Fig. 3 Retrieved stents. The Xience 2.75x38 mm stent was once fully deployed and elongated into the proximal RCA. The Promus 2.5x38 mm stent was undeployed and bent in half upon retrieval using a multi-snare catheter. RCA: right coronary artery.

Fig. 4 Results of the in vitro maximal stretching test of two different types of stents. (A) is the stent with 3 connectors (Xience Xpedition, Abbott Vascular, Santa Clara, CA, USA) that was not fractured but rather elongated. (B) is the stent with 2 connectors (Promus Premier, Boston Scientific, MN, USA ) that was fractured into four segments.
Reference
-
1. Bolte J, Neumann U, Pfafferott C, et al. Incidence, management, and outcome of stent loss during intracoronary stenting. Am J Cardiol. 2001; 88:565–567.2. Brilakis ES, Best PJ, Elesber AA, et al. Incidence, retrieval methods, and outcomes of stent loss during percutaneous coronary intervention: a large single-center experience. Catheter Cardiovasc Interv. 2005; 66:333–340.3. Alomar ME, Michael TT, Patel VG, et al. Stent loss and retrieval during percutaneous coronary interventions: a systematic review and meta-analysis. J Invasive Cardiol. 2013; 25:637–641.4. Jang JH, Woo SI, Yang DH, Park SD, Kim DH, Shin SH. Successful coronary stent retrieval from the ascending aorta using a gooseneck snare kit. Korean J Intern Med. 2013; 28:481–485.5. Collins N, Horlick E, Dzavik V. Triple wire technique for removal of fractured angioplasty guidewire. J Invasive Cardiol. 2007; 19:E230–E234.6. Kim JY, Yoon J, Jung HS, et al. Broken guidewire fragment in the radio-brachial artery during transradial sheath placement: percutaneous retrieval via femoral approach. Yonsei Med J. 2005; 46:166–168.7. Kang JH, Rha SW, Lee DI, et al. Successful retrieval of a fractured and entrapped 0.035-inch terumo wire in the femoral artery using biopsy forceps. Korean Circ J. 2012; 42:201–204.8. Kim JH, Jang WJ, Ahn KJ, et al. Successful retrieval of intravascular stent remnants with a combination of rotational atherectomy and a gooseneck snare. Korean Circ J. 2012; 42:492–496.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques
- Removal of Dislodged Stent by Using 8 Fr Sheath and Forcep during Transradial Coronary Stenting
- Retrieval of a dislodged and dismounted coronary stent; using a rendezvous and snare technique at the brachial artery level via femoral approach
- Dislodgement of Two Stents in One Patient during Percutaneous Coronary Intervention
- Treatment of Stent Dislodgement Complicated by Coronary Artery Dissection using Parallel Wire Technique and Small Balloon
