Clin Nutr Res.
2016 Oct;5(4):279-289. 10.7762/cnr.2016.5.4.279.
A Study on the Dietary Intake and the Nutritional Status among the Pancreatic Cancer Surgical Patients
- Affiliations
-
- 1Department of Nutritional Science and Food Management, Ewha Womans University, Seoul 03760, Korea. nschang@ewha.ac.kr
- 2Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul 06273, Korea.
- 3Department of Nutrition Services, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul 06273, Korea.
- 4Department of Food and Nutrition, Soongeui Women’s College, Seoul 04628, Korea.
- 5Department of Nutrition Care, Severance Hospital, Seoul 03722, Korea. nutrpine@yuhs.ac
- KMID: 2355300
- DOI: http://doi.org/10.7762/cnr.2016.5.4.279
Abstract
- The adequate dietary intake is important to maintain the nutritional status of the patients after pancreatic cancer surgery. This prospective study was designed to investigate the dietary intake and the nutritional status of the patients who had pancreatic cancer surgery. Thirty-one patients (15 men, 16 women) were enrolled and measured body weight, body mass index (BMI), nutritional risk index (NRI), and Malnutrition Universal Screening Tool (MUST). Actual oral intake with nutritional impact symptoms recorded on the clinical research foam at every meal and medical information were collected from electronic medical charts. The rates of malnutrition at admission were 45.1% (14/31) and 28.9% (9/31) by NRI and MUST method, respectively, but those were increased to 87% (27/31) and 86.6% (26/31) after operation on discharge. The median values of daily intake of energy, carbohydrates, fat, and protein were 588.1 kcal, 96.0 g, 11.8 g, and 27.0 g, respectively. Most patients (n = 20, 64.5%) experienced two or more symptoms such as anorexia, abdominal bloating and early satiety. There were negative correlations between C-reactive protein (CRP) levels and the intake of total energy, protein, fat, and zinc. The rates of malnutrition were increased sharply after surgery and the dietary intake also influenced the inflammatory indicators. The results suggested that need of considering special therapeutic diets for the patients who received pancreatic surgery.
Keyword
MeSH Terms
Figure
-

Figure 1 Flow sheet of the enrollment. M, male; F, female; LOS, length of hospital
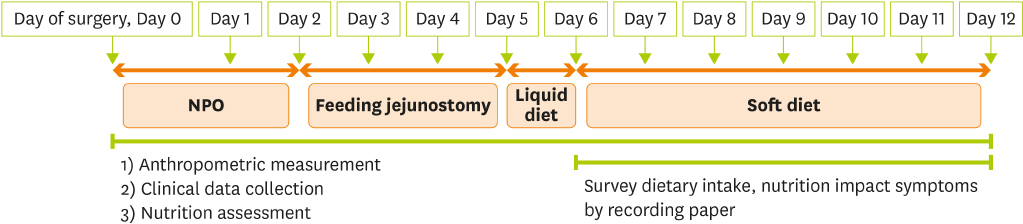
Figure 2 Scheduled diet orders for the subjects after pancreatic surgery. NPO, nothing by mouth.
Reference
-
1. Afaneh C, Gerszberg D, Slattery E, Seres DS, Chabot JA, Kluger MD. Pancreatic cancer surgery and nutrition management: a review of the current literature. Hepatobiliary Surg Nutr. 2015; 4:59–71.2. Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg. 2006; 244:10–15.
Article3. Gouma DJ, Nieveen van Dijkum EJ, Obertop H. The standard diagnostic work-up and surgical treatment of pancreatic head tumours. Eur J Surg Oncol. 1999; 25:113–123.
Article4. Gouma DJ, van Geenen RC, van Gulik TM, de Haan RJ, de Wit LT, Busch OR, Obertop H. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg. 2000; 232:786–795.
Article5. Shin JH, Han WK. A study of sixty consecutive whipple procedure by single surgeon. J Korean Surg Soc. 2004; 67:60–64.6. Bassi C, Falconi M, Salvia R, Mascetta G, Molinari E, Pederzoli P. Management of complications after pancreaticoduodenectomy in a high volume centre: results on 150 consecutive patients. Dig Surg. 2001; 18:453–457.
Article7. Cameron JL, He J. Two thousand consecutive pancreaticoduodenectomies. J Am Coll Surg. 2015; 220:530–536.
Article8. La Torre M, Ziparo V, Nigri G, Cavallini M, Balducci G, Ramacciato G. Malnutrition and pancreatic surgery: prevalence and outcomes. J Surg Oncol. 2013; 107:702–708.
Article9. Park JW, Jang JY, Kim EJ, Kang MJ, Kwon W, Chang YR, Han IW, Kim SW. Effects of pancreatectomy on nutritional state, pancreatic function and quality of life. Br J Surg. 2013; 100:1064–1070.
Article10. Muniz CK, Braga CB, Kemp R, Santos JS, Cunha SF. Clinical and nutritional status in the late postoperative of pancreaticoduodenectomy: influence of pylorus preservation procedure. Acta Cir Bras. 2012; 27:123–130.
Article11. Kim SH. Calculation of energy expenditure in patients undergoing pancreaticoduodenectomy [master's thesis]. Jeonju: Chonbuk National University;2013.12. Braga M, Pecorelli N, Ariotti R, Capretti G, Greco M, Balzano G, Castoldi R, Beretta L. Enhanced recovery after surgery pathway in patients undergoing pancreaticoduodenectomy. World J Surg. 2014; 38:2960–2966.
Article13. Goonetilleke KS, Hathurusinghe HR, Burden S, Siriwardena AK. Nutritional and anthropometric assessment of the scope for dietary optimization during staging prior to pancreaticoduodenectomy. JOP. 2008; 9:415–421.14. Niedergethmann M, Shang E, Farag Soliman M, Saar J, Berisha S, Willeke F, Post S. Early and enduring nutritional and functional results of pylorus preservation vs classic Whipple procedure for pancreatic cancer. Langenbecks Arch Surg. 2006; 391:195–202.
Article15. Iqbal N, Lovegrove RE, Tilney HS, Abraham AT, Bhattacharya S, Tekkis PP, Kocher HM. A comparison of pancreaticoduodenectomy with pylorus preserving pancreaticoduodenectomy: a meta-analysis of 2822 patients. Eur J Surg Oncol. 2008; 34:1237–1245.
Article16. Carey S, Storey D, Biankin AV, Martin D, Young J, Allman-Farinelli M. Long term nutritional status and quality of life following major upper gastrointestinal surgery - a cross-sectional study. Clin Nutr. 2011; 30:774–779.
Article17. Fujii T, Yamada S, Murotani K, Okamura Y, Ishigure K, Kanda M, Takeda S, Morita S, Nakao A, Kodera Y. Oral food intake versus fasting on postoperative pancreatic fistula after distal pancreatectomy: a multi-institutional randomized controlled trial. Medicine (Baltimore). 2015; 94:e2398.18. Lee CY, Lee YJ, Whang S, Park KM, Choi DR, Kim KH, Lee SG. Comparison between a pylorus-preserving pancreatoduodenectomy and a classical pancreatoduodenectomy. J Korean Surg Soc. 2000; 58:85–93.19. Choi MG, Kim SW, Jang JY, Yoon YS, Park YH. Long-term functional outcome after pancreatoduodenectomy. Korean J Hepatobiliary Pancreat Surg. 2004; 8:20–30.20. McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009; 12:223–226.
Article21. Akizuki E, Kimura Y, Nobuoka T, Imamura M, Nagayama M, Sonoda T, Hirata K. Reconsideration of postoperative oral intake tolerance after pancreaticoduodenectomy: prospective consecutive analysis of delayed gastric emptying according to the ISGPS definition and the amount of dietary intake. Ann Surg. 2009; 249:986–994.
Article22. Bae JM, Park JW, Yang HK, Kim JP. Nutritional status of gastric cancer patients after total gastrectomy. World J Surg. 1998; 22:254–260.
Article23. Hwang SE, Jung MJ, Cho BH, Yu HC. Clinical feasibility and nutritional effects of early oral feeding after pancreaticoduodenectomy. Korean J Hepatobiliary Pancreat Surg. 2014; 18:84–89.
Article24. Warren J, Bhalla V, Cresci G. Postoperative diet advancement: surgical dogma vs evidence-based medicine. Nutr Clin Pract. 2011; 26:115–125.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes in Dietary Intake, Body Weight, Nutritional Status, and Metabolic Rate in a Pancreatic Cancer Patient
- A Study of Dietary Intakes and Nutritional Status after Total Gastrectomy of Early Gastric Cancer Patients
- Effects of Individualized Nutritional Education Programs on the Level of Nutrient Intake and Nutritional Status of Colorectal Cancer Patients Undergoing Palliative Chemotherapy
- Nutrients Intake, Zinc Status and Health Risk Factors in Elderly Korean Women as Evaluated by the Nutrition Screening Inistiative (NSI) Checklist
- Nutritional Intake and Postoperative Pulmonary Complications among Lung Cancer Patients who Underwent Pulmonary Resection
