Primary Intraosseus Xanthoma Involving the Proximal Femur in a Normolipidemic Patient: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Korea.
- 2Department of Orthopaedic Surgery, Pusan National University Hospital, Pusan National University School of Medicine, Korea. namhoonmoon@gmail.com
- KMID: 2354552
- DOI: http://doi.org/10.5371/hp.2016.28.3.182
Abstract
- We report the case of a 25-year-old woman presenting with left hip pain. A lesion was found in the proximal femoral metaphysis. Benign bone tumor, such as intraosseous lipoma or liposclerosing myxofibrous tumor, was suspected based on simple radiographs and magnetic resonance images. Curettage of the lesion and bone grafting was performed. Histologic findings reflected primary intraosseous xanthoma of the proximal femur. Laboratory tests revealed the patient to be normolipidemic, while immunoelectrophoretic fractionation of lipoproteins revealed normal values for alpha, pre-beta, beta, and chylomicrons. At the one-year follow-up, there was no evidence of local recurrence. This is the first reported case of primary intraosseous xanthoma of the proximal femur in a normolipidemic patient.
MeSH Terms
Figure
-

Fig. 1 Preoperative radiograph, showing a large osteolytic lesion with well-defined margins in the proximal metaphysis of the femur, partially surrounded by sclerotic cortical bone.
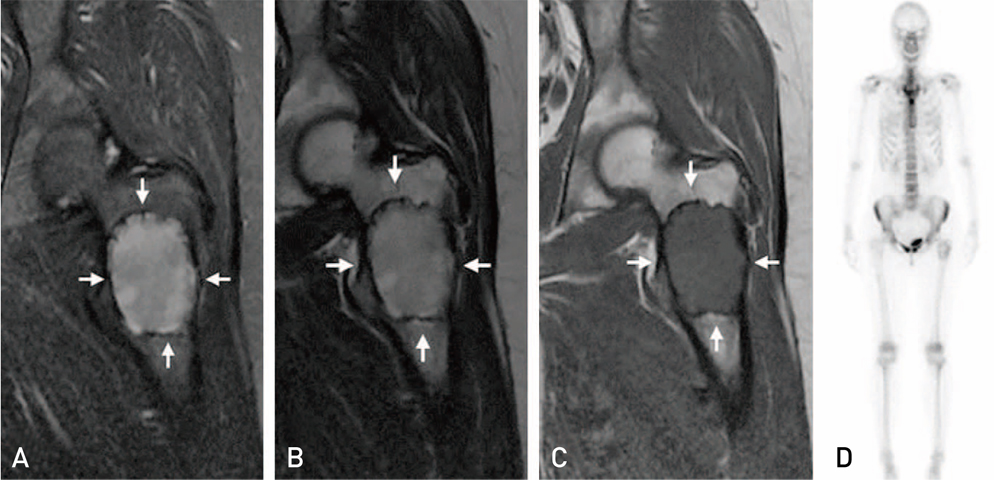
Fig. 2 Magnetic resonance images, showing a well-demarcated intra-osseous lesion measuring 58×42×42 mm. (A) Fat-suppressed image. (B) Fast spin-echo T2-weighted image. (C) T1-weighted image. (D) Radionuclide bone scan.

Fig. 3 Postoperative radiograph, showing curettage and bone grafting with a femoral head allograft. Prophylactic internal fixation was performed to prevent fracture.

Fig. 4 Histopathologic results (hematoxylin and eosin stain, ×200). The lesion shows heavy infiltration of foamy histiocytes (arrows).

Fig. 5 One-year follow-up radiograph, showing removal of the implant and no progression of the osteolytic lesion.
Reference
-
1. Ali S, Fedenko A, Syed AB, et al. Bilateral primary xanthoma of the humeri with pathologic fractures: A case report. World J Radiol. 2013; 5:345–348.
Article2. Dallari D, Marinelli A, Pellacani A, et al. Xanthoma of bone: first sign of hyperlipidemia type IIB: a case report. Clin Orthop Relat Res. 2003; (410):274–277.3. Boisgard S, Bringer O, Aufauvre B, et al. Intraosseous xanthoma without lipid disorders Case-report and literature review. Joint Bone Spine. 2000; 67:71–74.4. Kovac A, Kuo YZ, Sagar V. Radiographic and radioisotope evaluation of intra-osseous xanthoma. Br J Radiol. 1976; 49:281–285.
Article5. Yamamoto T, Kawamoto T, Marui T, et al. Multimodality imaging features of primary xanthoma of the calcaneus. Skeletal Radiol. 2003; 32:367–370.
Article6. Bertoni F, Unni KK, McLeod RA, Sim FH. Xanthoma of bone. Am J Clin Pathol. 1988; 90:377–384.
Article7. Huang CF, Cheng SN, Hung CH, et al. Xanthoma of bone in a normolipidemic child: report of one case. Acta Paediatr Taiwan. 2000; 41:158–160.8. Sobti A, Agrawal P, Agarwala S, Agarwal M. Giant cell tumor of bone - an overview. Arch Bone Jt Surg. 2016; 4:2–9.9. Kapukaya A, Subasi M, Dabak N, Ozkul E. Osseous lipoma: eleven new cases and review of the literature. Acta Orthop Belg. 2006; 72:603–614.10. Hamilton WC, Ramsey PL, Hanson SM, Schiff DC. Osseous xanthoma and multiple hand tumors as a complication of hyperlipidemia. Report of a case. J Bone Joint Surg Am. 1975; 57:551–553.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Xanthomas of the Bilateral Achilles Tendon in a Normolipidemic Patient
- Generalized Plane Xanthoma Associated with Monoclonal Gammopathy of Unknown Significance
- A Case of Type IV Hyperlipoproteinemia with Palmar Xanthoma, Tuberous Xanthoma, and Eruptive Xanthoma
- A Case of Type IIb Hyperlipoproteinemia with Xanthoma Tuberosum, Xanthoma Planum and Xanthoma Striatum Palmare
- Solitary Bone Cyst of the Proximal Femur Mimicking Fibrous Dysplasia: A Case Report
