Clinical Evaluation of Functional Vision of +1.5 Diopters near Addition, Aspheric, Rotational Asymmetric Multifocal Intraocular Lens
- Affiliations
-
- 1International Vision Correction and Research Centre & David J Apple International Laboratory on Ocular Pathology, Department of Ophthalmology, University of Heidelberg, Heidelberg, Germany. E-mail@florian-kretz.de
- 2International Vision Correction Research Centre Network, Heidelberg, Germany.
- 3Eye-Clinic Ahaus-Raesfeld-Rheine, Gerl Group, Ahaus, Germany.
- KMID: 2353832
- DOI: http://doi.org/10.3341/kjo.2016.30.5.382
Abstract
- PURPOSE
To evaluate postoperative outcomes and visual performance in intermediate distance after implantation of a +1.5 diopters (D) addition, aspheric, rotational asymmetric multifocal intraocular lens (MIOL).
METHODS
Patients underwent bilateral cataract surgery with implantation of an aspheric, asymmetric MIOL with +1.5 D near addition. A complete ophthalmological examination was performed preoperatively and 3 months postoperatively. The main outcome measures were monocular and binocular uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), uncorrected intermediate visual acuity (UIVA), distance corrected intermediate visual acuity (DCIVA), uncorrected near visual acuity (UNVA) and distance corrected keratometry, and manifest refraction. The Salzburg Reading Desk was used to analyze unilateral and bilateral functional vision with uncorrected and corrected reading acuity, reading distance, reading speed, and the smallest log-scaled print size that could be read effectively at near and intermediate distances.
RESULTS
The study comprised 60 eyes of 30 patients (mean age, 68.30 ± 9.26 years; range, 34 to 80 years). There was significant improvement in UDVA and CDVA. Mean UIVA was 0.01 ± 0.09 logarithm of the minimum angle of resolution (logMAR) and mean DCIVA was -0.02 ± 0.11 logMAR. In Salzburg Reading Desk analysis for UIVA, the mean subjective intermediate distance was 67.58 ± 8.59 cm with mean UIVA of -0.02 ± 0.09 logMAR and mean word count of 96.38 ± 28.32 words/min.
CONCLUSIONS
The new aspheric, asymmetric, +1.5 D near addition MIOL offers good results for distance visual function in combination with good performance for intermediate distances and functional results for near distance.
Keyword
MeSH Terms
Figure
-
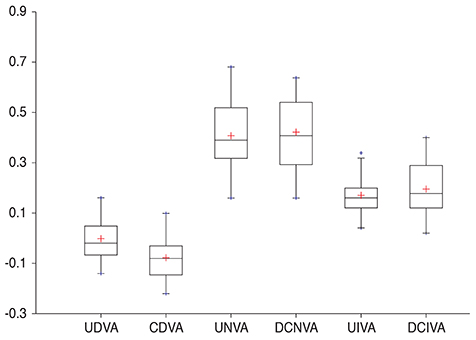
Fig. 1 Postoperative visual acuities. UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; UNVA = uncorrected near visual acuity; DCNVA = distance corrected near visual acuity; UIVA = uncorrected intermediate visual acuity; DCIVA = distance corrected intermediate visual acuity.
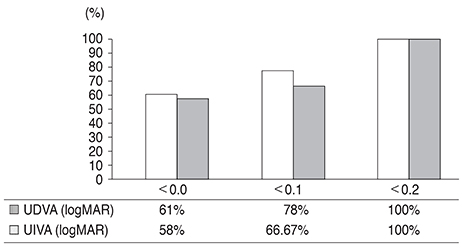
Fig. 2 Cumulative binocular visual acuity for distance and intermediate. UDVA = uncorrected distance visual acuity; logMAR = logarithm of the minimum angle of resolution; UIVA = uncorrected intermediate visual acuity.
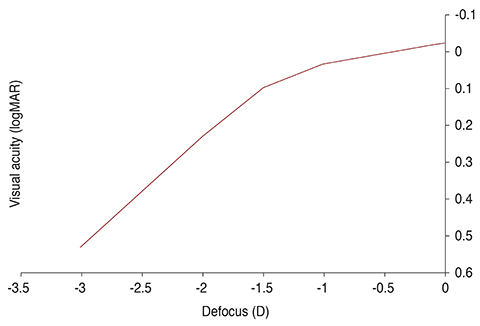
Fig. 3 Monocular defocus curve (logarithm of the minimum angle of resolution, logMAR). D = diopters.
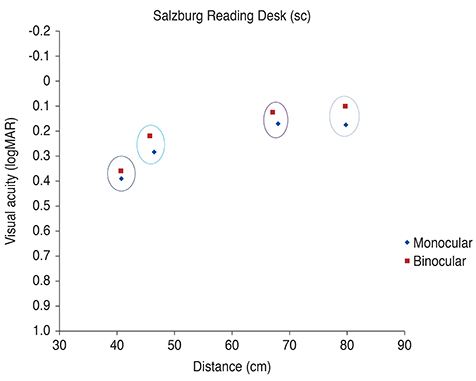
Fig. 4 Uncorrected visual acuity for near and intermediate distance evaluated with Salzburg Reading Desk. logMAR = logarithm of the minimum angle of resolution; sc = sine correctione (unccoreccted).
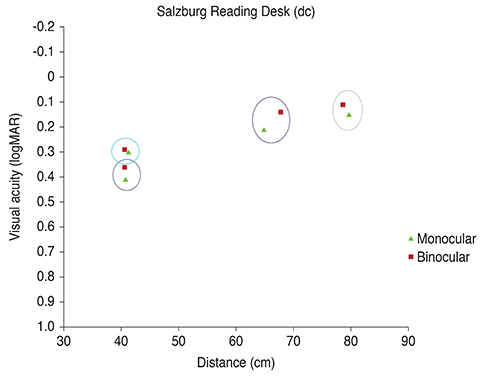
Fig. 5 Distance corrected visual acuity for near and intermediate distance evaluated with Salzburg Reading Desk. logMAR = logarithm of the minimum angle of resolution; dc = distance corrected.
Reference
-
1. Olsen T, Funding M. Ray-tracing analysis of intraocular lens power in situ. J Cataract Refract Surg. 2012; 38:641–647.2. Cochener B, Vryghem J, Rozot P, et al. Visual and refractive outcomes after implantation of a fully diffractive trifocal lens. Clin Ophthalmol. 2012; 6:1421–1427.3. Gatinel D, Houbrechts Y. Comparison of bifocal and trifocal diffractive and refractive intraocular lenses using an optical bench. J Cataract Refract Surg. 2013; 39:1093–1099.4. Mojzis P, Pena-Garcia P, Liehneova I, et al. Outcomes of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2014; 40:60–69.5. Sheppard AL, Shah S, Bhatt U, et al. Visual outcomes and subjective experience after bilateral implantation of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2013; 39:343–349.6. Voskresenskaya A, Pozdeyeva N, Pashtaev N, et al. Initial results of trifocal diffractive IOL implantation. Graefes Arch Clin Exp Ophthalmol. 2010; 248:1299–1306.7. Alio JL, Plaza-Puche AB, Montalban R, Javaloy J. Visual outcomes with a single-optic accommodating intraocular lens and a low-addition-power rotational asymmetric multifocal intraocular lens. J Cataract Refract Surg. 2012; 38:978–985.8. Dexl AK, Schlogel H, Wolfbauer M, Grabner G. Device for improving quantification of reading acuity and reading speed. J Refract Surg. 2010; 26:682–688.9. Khoramnia R, Auffarth GU, Rabsilber TM, Holzer MP. Implantation of a multifocal toric intraocular lens with a surface-embedded near segment after repeated LASIK treatments. J Cataract Refract Surg. 2012; 38:2049–2052.10. Thomas BC, Auffarth GU, Philips R, et al. Clinical results after implantation of a new segmental refractive multifocal intraocular lens. Ophthalmologe. 2013; 110:1058–1062.11. Bellucci R. Multifocal intraocular lenses. Curr Opin Ophthalmol. 2005; 16:33–37.12. Toto L, Falconio G, Vecchiarino L, et al. Visual performance and biocompatibility of 2 multifocal diffractive IOLs: six-month comparative study. J Cataract Refract Surg. 2007; 33:1419–1425.13. Kretz FT, Gerl M, Gerl R, et al. Clinical evaluation of a new pupil independent diffractive multifocal intraocular lens with a +2.75 D near addition: a European multicentre study. Br J Ophthalmol. 2015; 99:1655–1659.14. Kretz FT, Koss MJ, Auffarth GU. ZLB00 Study Group. Intermediate and near visual acuity of an aspheric, bifocal, diffractive multifocal intraocular lens with +3.25 D near addition. J Refract Surg. 2015; 31:295–299.15. Lesieur G. Outcomes after implantation of a trifocal diffractive IOL. J Fr Ophtalmol. 2012; 35:338–342.16. Lichtinger A, Rootman DS. Intraocular lenses for presbyopia correction: past, present, and future. Curr Opin Ophthalmol. 2012; 23:40–46.17. Kretz FT, Attia MA, Linz K, Auffarth GU. Level of binocular pseudoaccommodation in patients implanted with an apodised, diffractive and trifocal multifocal intraocular lens. Klin Monbl Augenheilkd. 2015; 232:947–952.18. Gatinel D, Pagnoulle C, Houbrechts Y, Gobin L. Design and qualification of a diffractive trifocal optical profile for intraocular lenses. J Cataract Refract Surg. 2011; 37:2060–2067.19. Venter JA, Pelouskova M, Collins BM, et al. Visual outcomes and patient satisfaction in 9366 eyes using a refractive segmented multifocal intraocular lens. J Cataract Refract Surg. 2013; 39:1477–1484.20. Gundersen KG, Potvin R. Comparative visual performance with monofocal and multifocal intraocular lenses. Clin Ophthalmol. 2013; 7:1979–1985.21. Radner W, Obermayer W, Richter-Mueksch S, et al. The validity and reliability of short German sentences for measuring reading speed. Graefes Arch Clin Exp Ophthalmol. 2002; 240:461–467.22. Alio JL, Grabner G, Plaza-Puche AB, et al. Postoperative bilateral reading performance with 4 intraocular lens models: six-month results. J Cataract Refract Surg. 2011; 37:842–852.23. Rasp M, Bachernegg A, Seyeddain O, et al. Bilateral reading performance of 4 multifocal intraocular lens models and a monofocal intraocular lens under bright lighting conditions. J Cataract Refract Surg. 2012; 38:1950–1961.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Aspheric Doublet Lens
- Comparison of Wavefront Analysis and Visual Function Between Monofocal and Multifocal Aspheric Intraocular Lenses
- Clinical Result of One-Piece Aspheric Intraocular Lens in Mild Zonule-Weakness
- Clinical Results of 3M Multifocal Intraocular Lens
- Comparison of Nd:YAG Capsulotomy Rates between Spherical and Aspheric Intraocular Lenses
