Clinical Effectiveness and Nephrotoxicity of Aerosolized Colistin Treatment in Multidrug-Resistant Gram-Negative Pneumonia
- Affiliations
-
- 1Research Institute of Clinical Medicine, Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Korea. lhbmd@jbnu.ac.kr
- 2Department of Pharmacy, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
- 3Department of Critical Care Medicine, Samsung medical Center, School of Medicine, Sungkyunkwan University, Seoul, Korea.
- KMID: 2350905
- DOI: http://doi.org/10.4266/kjccm.2016.00129
Abstract
- BACKGROUND
Colistin (polymyxin E) is active against multidrug-resistant Gram-negative bacteria (MDR-GNB). However, the effectiveness of inhaled colistin is unclear. This study was designed to assess the effectiveness and safety of aerosolized colistin for the treatment of ventilator-associated pneumonia (VAP) caused by MDR-GNB.
METHODS
In this retrospective longitudinal study, we evaluated the medical records of 63 patients who received aerosolized colistin treatment for VAP caused by MDR-GNB in the medical intensive care unit (MICU) from February 2012 to March 2014.
RESULTS
A total of 25 patients with VAP caused by MDR-GNB were included in this study. The negative conversion rate was 84.6% after treatment, and acute kidney injury (AKI) occurred in 11 patients (44%, AKI group). The average length of MICU stay and colistin treatment- related factors, such as daily and total cumulative doses and administration period, were not significantly different between groups. In-hospital mortality tended to be higher in the AKI group (p = 0.07). Multivariate analysis showed that a body mass index less than 18 was an independent risk factor of mortality (odds ratio [OR] = 21.95, 95% confidence interval [CI] 1.59-302.23; p = 0.02). Notably, AKI occurrence was closely related to the administration of more than two nephrotoxic drugs combined with aerosolized colistin (OR = 15.03, 95% CI 1.40-161.76; p = 0.025) and septic shock (OR = 8.10, 95% CI 1.40-161.76; p = 0.04).
CONCLUSIONS
The use of adjunctive aerosolized colistin treatment appears to be a relatively safe and effective option for the treatment of VAP caused by MDR-GNB. However, more research on the concomitant use of nephrotoxic drugs with aerosolized colistin will be necessary, as this can be an important risk factor of development of AKI.
MeSH Terms
-
Acute Kidney Injury
Body Mass Index
Colistin*
Drug Resistance, Microbial
Gram-Negative Bacteria
Hospital Mortality
Humans
Intensive Care Units
Longitudinal Studies
Medical Records
Mortality
Multivariate Analysis
Pneumonia*
Pneumonia, Ventilator-Associated
Retrospective Studies
Risk Factors
Shock, Septic
Treatment Outcome*
Colistin
Figure
-
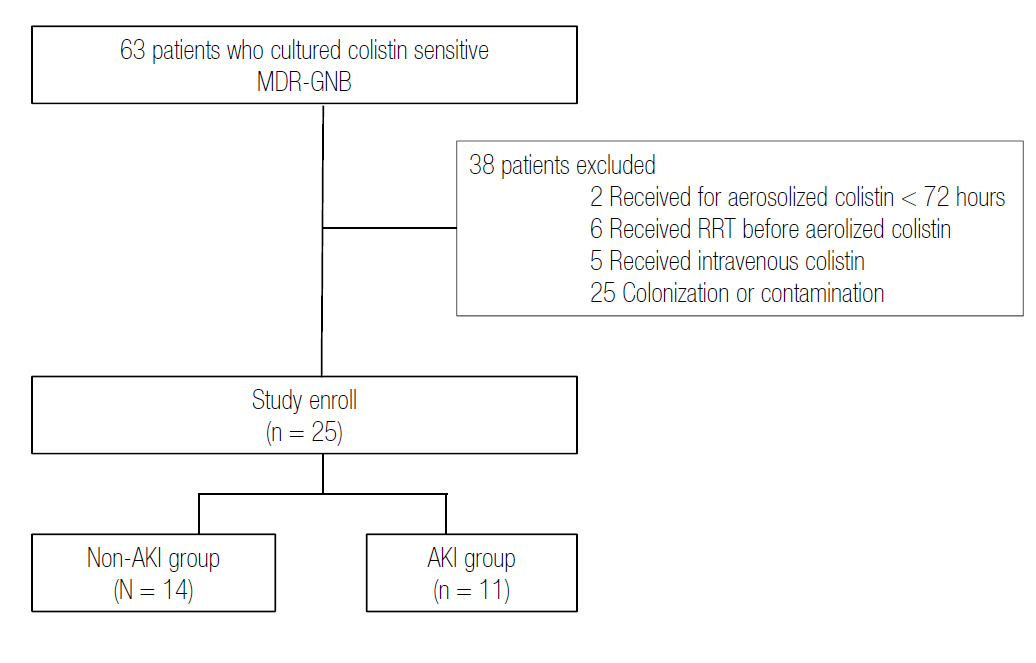
Fig. 1. Flow of patient screening and enrollment. MDR-GNB: multidrug-resistant Gram-negative bacteria; RRT: renal replacement therapy; AKI: acute kidney injury.
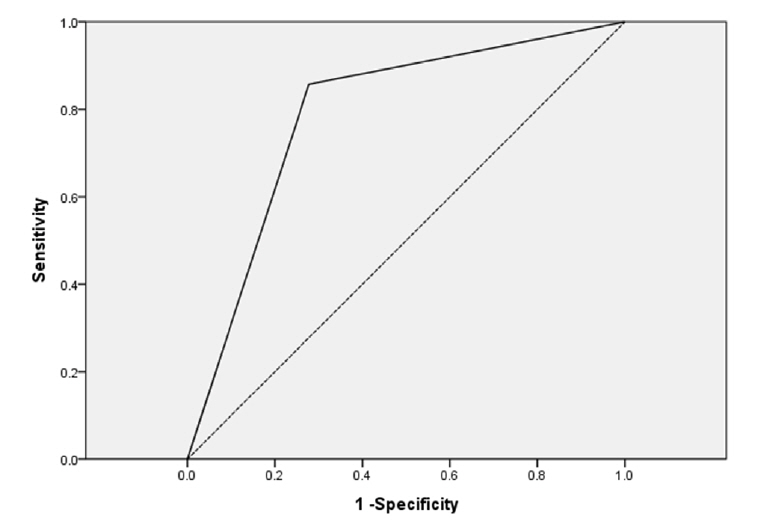
Fig. 2. The area under a ROC curve to predict factors associated with mortality and AKI. For mortality, the area under the ROC curve was 0.817 for patients with a body mass index <18 kg/m2 (p = 0.015). ROC: receiver operating characteristic; AKI: acute kidney injury.

Fig. 3. Relationship between the occurrence of AKI and concomitant use of nephrotoxic drugs, excluding vasopressors. Use of more than two nephrotoxic drugs concomitant with aerosolized colistin therapy increases the likelihood of developing AKI. AKI: acute kidney injury.
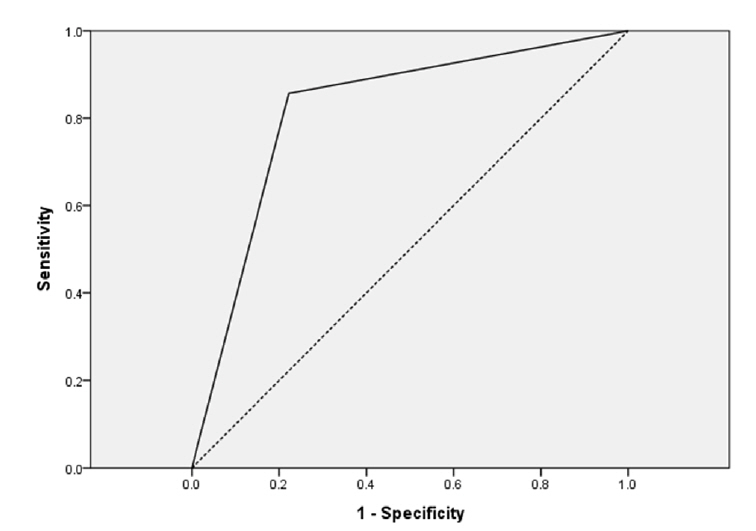
Fig. 4. The area under a ROC curve to predict factors associated with mortality and AKI. For AKI, the area under the ROC curve was 0.790 for patients who used more than two nephrotoxic drugs concomitant with aerosolized colistin (p = 0.027). ROC: receiver operating characteristic; AKI: acute kidney injury.
Reference
-
References
1. Hancock RE. Peptide antibiotics. Lancet. 1997; 349:418–22.
Article2. Falagas ME, Kasiakou SK. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin Infect Dis. 2005; 40:1333–41.
Article3. Falagas ME, Kasiakou SK. Toxicity of polymyxins: a systematic review of the evidence from old and recent studies. Crit Care. 2006; 10:R27.4. Pogue JM, Lee J, Marchaim D, Yee V, Zhao JJ, Chopra T, et al. Incidence of and risk factors for colistinassociated nephrotoxicity in a large academic health system. Clin Infect Dis. 2011; 53:879–84.
Article5. Hartzell JD, Neff R, Ake J, Howard R, Olson S, Paolino K, et al. Nephrotoxicity associated with intravenous colistin (colistimethate sodium) treatment at a tertiary care medical center. Clin Infect Dis. 2009; 48:1724–8.
Article6. Yapa SWS, Li J, Patel K, Wilson JW, Dooley MJ, George J, et al. Pulmonary and systemic pharmacokinetics of inhaled and intravenous colistin methanesulfonate in cystic fibrosis patients: targeting advantage of inhalational administration. Antimicrob Agents Chemother. 2014; 58:2570–9.7. Jensen T, Pedersen SS, Garne S, Heilmann C, Høiby N, Koch C. Colistin inhalation therapy in cystic fibrosis patients with chronic Pseudomonas aeruginosa lung infection. J Antimicrob Chemother. 1987; 19:831–8.8. Kollef MH, Niederman MS. Why is Acinetobacter baumannii a problem for critically ill patients? Intensive Care Med. 2015; 41:2170–2.9. Bogović TZ, Budimir A, Bošnjak Z, Hrabač P, Baronica R, Tomašević B, et al. Inhalation plus intravenous colistin versus intravenous colistin alone for treatment of ventilator associated pneumonia. Signa Vitae. 2014; 9(Suppl 1):29–33.10. Gurjar M. Colistin for lung infection: an update. J Intensive Care. 2015; 3:3.
Article11. Pogue JM, Lee J, Marchaim D, Yee V, Zhao JJ, Chopra T, et al. Incidence of and risk factors for colistin-associated nephrotoxicity in a large academic health system. Clin Infect Dis. 2011; 53:879–84.
Article12. Kaye KS, Kaye D. Polymyxins (polymyxin B and colistin). Principles and practice of infectious diseases. 6th ed. In : Mandell GL, Bennett JE, Dolin R, editors. Philadelphia: Elsevier;2005. p. 435–6.13. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008; 36:309–32.
Article14. Korbila IP, Michalopoulos A, Rafailidis PI, Nikita D, Samonis G, Falagas ME. Inhaled colistin as adjunctive to intravenous colistin for the treatment of microbiologically documented VAP: a comparative cohort study. Clin Microbiol Infect. 2010; 16:1230–6.15. Knaus W, Draper E, Wagner D, Zimmerman J. APACHE II: a severity of disease classification system. Crit Care Med. 1985; 13:818–29.16. Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis. 1991; 143:1121–9.
Article17. Kofteridis DP, Alexopoulou C, Valachis A, Maraki S, Dimopoulou D, Georgopoulos D, Samonis G. Aerosolized plus intravenous colistin versus intravenous colistin alone for the treatment of ventilatorassociated pneumonia: a matched case-control study. Clinical Infect Dis. 2010; 51:1238–44.
Article18. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A New Equation to Estimate Glomerular Filtration Rate. Ann Intern Med. 2009; 150:604–12.
Article19. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P; Acute Dialysis Quality Initiative work-group. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004; 8:R204–12.20. Hamer DH. Treatment of nosocomial pneumonia and tracheobronchitis caused by multidrug-resistant Pseudomonas aeruginosa with aerosolized colistin. Am J Respir Crit Care Med. 2000; 162:328–30.21. Evans ME, Feola DJ, Rapp RP. Polymyxin B sulfate and colistin: old antibi-otics for emerging multiresistant gram-negative bacteria. Ann Pharmacother. 1999; 33:960–7.
Article22. DeRyke CA, Crawford AJ, Uddin N, Wallace MR. Colistin dosing and nephrotoxicity in a large community teaching hospital. Antimicrob Agents Chemother. 2010; 54:4503–5.
Article23. Imberti R, Cusato M, Villani P, Carnevale L, Iotti GA, Langer M, et al. Steady-state pharmacokinetics and BAL concentration of colistin in critically Ill patients after IV colistin methanesulfonate administration. Chest. 2010; 138:1333–9.
Article24. Steinfort DP, Steinfort C. Effect of long-term nebulized colistin on lung function and quality of life in patients with chronic bronchial sepsis. Intern Med J. 2007; 37:495–8.
Article25. Marchand S, Bouchene S, de Monte M, Guilleminault L, Montharu J, Cabrera M, et al. Pharmacokinetics of Colistin Methansulphonate (CMS) and Colistin after CMS Nebulisation in Baboon Monkeys. Pharm Res. 2015; 32:3404–14.
Article26. Sorlí L, Luque S, Grau S, Berenguer N, Segura C, Montero MM, et al. Trough colistin plasma level is an independent risk factor for nephrotoxicity: a prospective observational cohort study. BMC Infect Dis. 2013; 13:380–8.
Article27. Katzmarzyk PT, Reeder BA, Elliott S, Joffres MR, Pahwa P, Raine KD, et al. Body mass index and risk of cardiovascular disease, cancer and all-cause mortality. Can J Public Health. 2012; 103:147–51.
Article28. O’Brien JM Jr, Welsh CH, Fish RH, Ancukiewicz M, Kramer AM. Excess body weight is not independently associated with outcome in mechanically ventilated patients with acute lung injury. Ann Intern Med. 2004; 140:338–45.
Article29. Hogue CW Jr, Stearns JD, Colantuoni E, Robinson KA, Stierer T, Mitter N, et al. The impact of obesity on outcomes after critical illness: a meta-analysis. Intensive Care Med. 2009; 35:1152–70.
Article30. Arabi YM, Dara SI, Tamim HM, Rishu AH, Bouchama A, et al. The Cooperative Antimicrobial Therapy of Septic Shock (CATSS) Data-base Research Group. Clinical characteristics, sepsis interventions and outcomes in the obese patients with septic shock: an international multicenter cohort study. Crit Care. 2013; 17:R72.31. Alothman GA, Ho B, Alsaadi MM, Ho SL, O’Drowsky L, Louca E, et al. Bronchial constriction and inhaled colistin in cystic fibrosis. Chest. 2005; 127:522–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Inhaled Colistin for Treatment of Pneumonia due to Colistin-Only-Susceptible Acinetobacter baumannii
- A Trial of Aerosolized Colistin for the Treatment of Nosocomial Pneumonia due to Multidrug-resistant Acinetobacter baumannii
- Treatment of drug resistant bacteria: new bugs, old drugs, and new therapeutic approaches
- Aerosolized antibiotics in the treatment of hospital-acquired pneumonia/ventilator-associated pneumonia
- Effects of Aerosol Colistin Treatment of Pneumonia Caused by Multi-drug Resistant Acinetobacter baumannii
