Ann Surg Treat Res.
2016 Sep;91(3):127-132. 10.4174/astr.2016.91.3.127.
Use of fibrin glue in preventing pseudorecurrence after laparoscopic total extraperitoneal repair of large indirect inguinal hernia
- Affiliations
-
- 1Department of General Surgery, Faculty of Medicine, Turgut Ozal University, Ankara, Turkey. murat05ozgur@hotmail.com
- 2Department of General Surgery, Ankara Training and Research Hospital, Ankara, Turkey.
- 3Department of Radiology, Ankara Training and Research Hospital, Ankara, Turkey.
- 4Department of Statistics, Faculty of Science, Hacettepe University, Ankara, Turkey.
- KMID: 2350539
- DOI: http://doi.org/10.4174/astr.2016.91.3.127
Abstract
- PURPOSE
Seroma is among the most common complications of laparoscopic total extraperitoneal (TEP) for especially large indirect inguinal hernia, and may be regarded as a recurrence by some patients. A potential area localized behind the mesh and extending from the inguinal cord into the scrotum may be one of the major etiological factors of this complication. Our aim is to describe a novel technique in preventing pseudorecurrence by using fibrin sealant to close that potential dead space.
METHODS
Forty male patients who underwent laparoscopic TEP for indirect inguinal hernia with at least 100-mL volume were included in this prospective clinical study. While fibrin sealant was used to close the potential dead space in the study group, nothing was used in the control group. The volume of postoperative fluid collection on ultrasound was compared between the groups.
RESULTS
Patient characteristics and the volumes of hernia sac were similar between the 2 groups. The mean volume of postoperative fluid collection was found as 120.2 mL in the control group and 53.7 mL in the study group, indicating a statistical significance (P < 0.001).
CONCLUSION
Minimizing the potential dead space with a fibrin sealant can reduce the amount of postoperative fluid collection, namely the incidence of pseudorecurrence.
Keyword
MeSH Terms
Figure
-
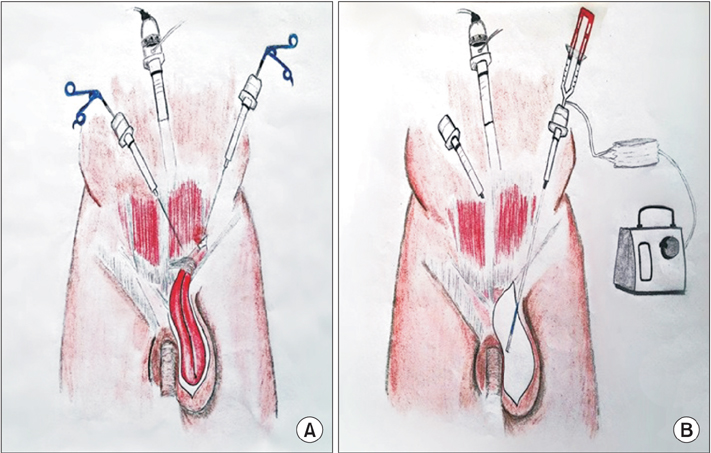
Fig. 1 (A) A drawing showing the placement of the trocars in a patient of study group. (B) Application of fibrin sealant into the potential dead space by using a laparoscopic applicator through the trocar near the anterior superior iliac spine.

Fig. 2 The image of a pseudorecurrence following laparoscopic total extraperitoneal for left scrotal hernia in a patient of control group.
Reference
-
1. Bringman S, Ramel S, Heikkinen TJ, Englund T, Westman B, Anderberg B. Tension-free inguinal hernia repair: TEP versus mesh-plug versus Lichtenstein: a prospective randomized controlled trial. Ann Surg. 2003; 237:142–147.2. Griffin KJ, Harris S, Tang TY, Skelton N, Reed JB, Harris AM. Incidence of contralateral occult inguinal hernia found at the time of laparoscopic trans-abdominal pre-peritoneal (TAPP) repair. Hernia. 2010; 14:345–349.3. Park BS, Ryu DY, Son GM, Cho YH. Factors influencing on difficulty with laparoscopic total extraperitoneal repair according to learning period. Ann Surg Treat Res. 2014; 87:203–208.4. Franneby U, Sandblom G, Nordin P, Nyren O, Gunnarsson U. Risk factors for long-term pain after hernia surgery. Ann Surg. 2006; 244:212–219.5. Bansal VK, Misra MC, Babu D, Victor J, Kumar S, Sagar R, et al. A prospective, randomized comparison of long-term outcomes: chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg Endosc. 2013; 27:2373–2382.6. Pahwa HS, Kumar A, Agarwal P, Agarwal AA. Current trends in laparoscopic groin hernia repair: A review. World J Clin Cases. 2015; 3:789–792.7. Wang WJ, Chen JZ, Fang Q, Li JF, Jin PF, Li ZT. Comparison of the effects of laparoscopic hernia repair and Lichtenstein tension-free hernia repair. J Laparoendosc Adv Surg Tech A. 2013; 23:301–305.8. McCormack K, Scott NW, Go PM, Ross S, Grant AM. EU Hernia Trialists Collaboration. Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev. 2003; (1):CD001785.9. O'Rourke MG, O'Rourke TR. Inguinal hernia: aetiology, diagnosis, post-repair pain and compensation. ANZ J Surg. 2012; 82:201–206.10. Katkhouda N, Mavor E, Friedlander MH, Mason RJ, Kiyabu M, Grant SW, et al. Use of fibrin sealant for prosthetic mesh fixation in laparoscopic extraperitoneal inguinal hernia repair. Ann Surg. 2001; 233:18–25.11. Lovisetto F, Zonta S, Rota E, Mazzilli M, Bardone M, Bottero L, et al. Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: a prospective, randomized study. Ann Surg. 2007; 245:222–231.12. Descottes B, Bagot d'Arc M. Fibrin sealant in inguinal hernioplasty: an observational multicentre study in 1,201 patients. Hernia. 2009; 13:505–510.13. Canonico S. The use of human fibrin glue in the surgical operations. Acta Biomed. 2003; 74:Suppl 2. 21–25.14. Zieren J, Castenholz E, Baumgart E, Müller JM. Effects of fibrin glue and growth factors released from platelets on abdominal hernia repair with a resorbable PGA mesh: experimental study. J Surg Res. 1999; 85:267–272.15. Schenk WG 3rd, Burks SG, Gagne PJ, Kagan SA, Lawson JH, Spotnitz WD. Fibrin sealant improves hemostasis in peripheral vascular surgery: a randomized prospective trial. Ann Surg. 2003; 237:871–876.16. Jenkins ED, Lerdsirisopon S, Costello KP, Melman L, Greco SC, Frisella MM, et al. Laparoscopic fixation of biologic mesh at the hiatus with fibrin or polyethylene glycol sealant in a porcine model. Surg Endosc. 2011; 25:3405–3413.17. Wilson C, Robinson S, French J, White S. Strategies to reduce pancreatic stump complications after open or laparoscopic distal pancreatectomy. Surg Laparosc Endosc Percutan Tech. 2014; 24:109–117.18. Chevrel JP, Rath AM. The use of fibrin glues in the surgical treatment of incisional hernias. Hernia. 1997; 1:9–14.19. Canonico S, Sciaudone G, Pacifico F, Santoriello A. Inguinal hernia repair in patients with coagulation problems: prevention of postoperative bleeding with human fibrin glue. Surgery. 1999; 125:315–317.20. Lau H. Fibrin sealant versus mechanical stapling for mesh fixation during endoscopic extraperitoneal inguinal hernioplasty: a randomized prospective trial. Ann Surg. 2005; 242:670–675.21. Ceccarelli G, Casciola L, Pisanelli MC, Bartoli A, Di Zitti L, Spaziani A, et al. Comparing fibrin sealant with staples for mesh fixation in laparoscopic transabdominal hernia repair: a case control-study. Surg Endosc. 2008; 22:668–673.22. Chan MS, Teoh AY, Chan KW, Tang YC, Ng EK, Leong HT. Randomized double-blinded prospective trial of fibrin sealant spray versus mechanical stapling in laparoscopic total extraperitoneal hernioplasty. Ann Surg. 2014; 259:432–437.23. Damiano G, Gioviale MC, Palumbo VD, Spinelli G, Buscemi S, Ficarella S, et al. Human fibrin glue sealing versus suture polypropylene fixation in Lichtenstein inguinal herniorrhaphy: a prospective observational study. Chirurgia (Bucur). 2014; 109:660–663.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Totally Extraperitoneal Laparoscopic Repair of Obturator Hernia withPartial Intestinal Obstruction
- Totally Extraperitoneal (TEP) Approach for Femoral Hernia
- Short-term comparative study of three-dimensional and two-dimensional laparoscopic surgery for total extraperitoneal primary inguinal hernia repair
- Percutaneous Internal Ring Suturing for Indirect Inguinal Hernia in Pediatric Patients
- To Minimize Post-operative Pain in Inguinal Hernia Repair: Single-port Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair without Fixation of the Mesh
