Morphological and Electrical Characteristics in Patient with Hypertrophic Cardiomyopathy: Quantitative Analysis of 864 Korean Cohort
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. oys@catholic.ac.kr
- 2Department of Cardiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 2345877
- DOI: http://doi.org/10.3349/ymj.2015.56.6.1515
Abstract
- PURPOSE
Although several studies have reported the morphological and electrical characteristics in patients with hypertrophic cardiomyopathy (HCM), comparison between asymmetric and apical HCM has not been investigated in a reasonably sized cohort.
MATERIALS AND METHODS
Echocardiography and electrocardiography were quantitatively analyzed in patients with HCM in a Korean tertiary referral center.
RESULTS
Of 864 patients (mean age 55.4+/-14.2 years, 68.9% men), 255 (29.5%) patients had apical HCM, 553 (64.0%) patients asymmetric HCM, and 56 (6.4%) patients mixed type HCM. In echocardiographic evaluations, about three quarters of patients (75.8%) had left atrial enlargement. Left ventricular (LV) dilatations and systolic dysfunction were observed in 6.1% and 2.4%, respectively. QRS widening, PR prolongation, and pathologic Q wave are frequent in patients with asymmetric HCM, while LV strain is frequent in patient with apical HCM. The prevalence of J-point elevations (9.4% in inferior, 2.2% in lateral leads) were substantially higher than that in general population. Giant negative T wave was observed in 15.0% of total patients (32.2% in apical, 6.2% in asymmetric, 25% in mixed type). There was no significant correlation between the thickness of the apical wall and the amplitude of T wave inversion (r=-0.005, p=0.71).
CONCLUSION
In a large cohort of HCM including apical type, repolarization abnormalities, including early repolarization and QT prolongation as well as LV strain, were significantly observed. T wave inversion was not appropriate for screening of HCM and not correlated with apical wall thickness.
MeSH Terms
Figure
-

Fig. 1 Proportion of hypertrophic cardiomyopathy type relative to patient's age. In contrast to asymmetric hypertrophy, the proportion of patients with apical hypertrophy increased with age.
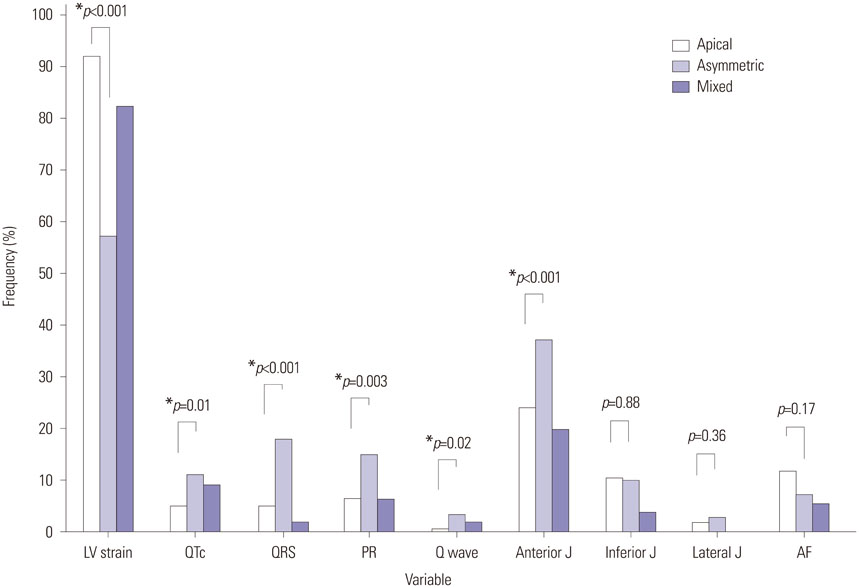
Fig. 2 Electrocardiographic abnormalities according to the type of hypertrophy. *Advanced electrical abnormalities such as QT prolongation, QRS widening, PR prolongation, and pathologic Q wave were more prevalent in patients with asymmetric hypertrophy. LV, left ventricle; QTc, corrected QT duration ≥480 msec; QRS, QRS duration ≥120 msec; PR, PR interval ≥200 msec; Q wave, pathologic Q wave; anterior J, J point in anterior leads ≥0.1 mV; inferior J, J point in inferior leads ≥0.1 mV; lateral J, J point in lateral leads ≥0.1 mV; AF, atrial fibrillation.
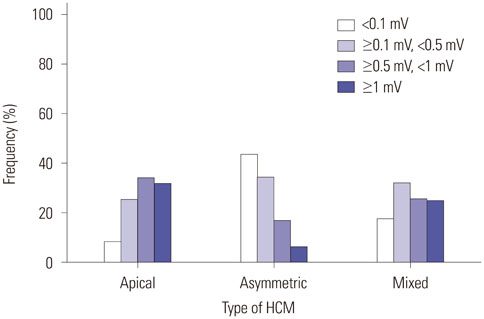
Fig. 3 The amplitude T wave inversion according to the type of hypertrophic cardiomyopathy. HCM, hypertrophic cardiomyopathy.

Fig. 4 Correlation between apical wall thickness and the amplitude of T wave inversion in patients with apical hypertrophy. No significant correlation was observed.
Reference
-
1. Abbasi AS, MacAlpin RN, Eber LM, Pearce ML. Echocardiographic diagnosis of idiopathic hypertrophic cardiomyopathy without outflow obstruction. Circulation. 1972; 46:897–904.
Article2. Henry WL, Clark CE, Epstein SE. Asymmetric septal hypertrophy. Echocardiographic identification of the pathognomonic anatomic abnormality of IHSS. Circulation. 1973; 47:225–233.3. Pridie RB, Oakley C. Mitral valve movement in hypertrophic obstructive cardiomyopathy. Br Heart J. 1969; 31:390.4. Sakamoto T, Tei C, Murayama M, Ichiyasu H, Hada Y. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle. Echocardiographic and ultrasono-cardiotomographic study. Jpn Heart J. 1976; 17:611–629.
Article5. Klues HG, Schiffers A, Maron BJ. Phenotypic spectrum and patterns of left ventricular hypertrophy in hypertrophic cardiomyopathy: morphologic observations and significance as assessed by two-dimensional echocardiography in 600 patients. J Am Coll Cardiol. 1995; 26:1699–1708.
Article6. Maron BJ, Wolfson JK, Ciró E, Spirito P. Relation of electrocardiographic abnormalities and patterns of left ventricular hypertrophy identified by 2-dimensional echocardiography in patients with hypertrophic cardiomyopathy. Am J Cardiol. 1983; 51:189–194.
Article7. Savage DD, Seides SF, Clark CE, Henry WL, Maron BJ, Robinson FC, et al. Electrocardiographic findings in patients with obstructive and nonobstructive hypertrophic cardiomyopathy. Circulation. 1978; 58(3 Pt 1):402–408.
Article8. Prescott R, Quinn JS, Littmann D. Electrocardiographic changes in hypertrophic subaortic stenosis which simulate myocardial infarction. Am Heart J. 1963; 66:42–48.
Article9. Cosio FG, Moro C, Alonso M, de la Calzada CS, Liovet A. The Q waves hypertrophic cardiomyopathy: an electrophysiologic study. N Engl J Med. 1980; 302:96–99.10. Maron BJ, Maron MS, Wigle ED, Braunwald E. The 50-year history, controversy, and clinical implications of left ventricular outflow tract obstruction in hypertrophic cardiomyopathy from idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomyopathy: from idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomyopathy. J Am Coll Cardiol. 2009; 54:191–200.
Article11. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, et al. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003; 42:1687–1713.
Article12. Yamaguchi H, Ishimura T, Nishiyama S, Nagasaki F, Nakanishi S, Takatsu F, et al. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): ventriculographic and echocardiographic features in 30 patients. Am J Cardiol. 1979; 44:401–412.
Article13. Chikamori T, Doi YL, Akizawa M, Yonezawa Y, Ozawa T, McKenna WJ. Comparison of clinical, morphological, and prognostic features in hypertrophic cardiomyopathy between Japanese and western patients. Clin Cardiol. 1992; 15:833–837.
Article14. Kim SH, Kim SO, Han S, Hwang KW, Lee CW, Nam GB, et al. Long-term comparison of apical versus asymmetric hypertrophic cardiomyopathy. Int Heart J. 2013; 54:207–211.
Article15. Eriksson MJ, Sonnenberg B, Woo A, Rakowski P, Parker TG, Wigle ED, et al. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002; 39:638–645.
Article16. Otto CM. The practice of clinical echocardiography. 2nd ed. Philadelphia: W.B. Saunders;2002. p. 589.17. Feigenbaum H, Armstrong WF, Ryan T. Feigenbaum's echocardiography. 6th ed. Philadelphia: Lippincott Williams & Wilkins;2005. p. 545.18. Romhilt DW, Bove KE, Norris RJ, Conyers E, Conradi S, Rowlands DT, et al. A critical appraisal of the electrocardiographic criteria for the diagnosis of left ventricular hypertrophy. Circulation. 1969; 40:185–195.
Article19. Wagner GS, Marriott HJL. Marriott's practical electrocardiography. 10th ed. Philadelphia: Lippincott Williams & Wilkins;2001. p. 90–93.20. Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995; 92:785–789.
Article21. Brock R. Functional obstruction of the left ventricle; acquired aortic subvalvar stenosis. Guys Hosp Rep. 1957; 106:221–238.22. Teare D. Asymmetrical hypertrophy of the heart in young adults. Br Heart J. 1958; 20:1–8.
Article23. Braunwald E, Lambrew CT, Rockoff SD, Ross J Jr, Morrow AG. Idiopathic hypertrophic subaortic stenosis. I. A description of the disease based upon an analysis of 64 patients. Circulation. 1964; 30:Suppl 4. 3–119.
Article24. Maron BJ, Bonow RO, Cannon RO 3rd, Leon MB, Epstein SE. Hypertrophic cardiomyopathy. Interrelations of clinical manifestations, pathophysiology, and therapy (2). N Engl J Med. 1987; 316:844–852.25. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002; 287:1308–1320.26. Louie EK, Maron BJ. Apical hypertrophic cardiomyopathy: clinical and two-dimensional echocardiographic assessment. Ann Intern Med. 1987; 106:663–670.
Article27. Ho CY, Sweitzer NK, McDonough B, Maron BJ, Casey SA, Seidman JG, et al. Assessment of diastolic function with Doppler tissue imaging to predict genotype in preclinical hypertrophic cardiomyopathy. Circulation. 2002; 105:2992–2997.
Article28. Maron BJ, Spirito P, Green KJ, Wesley YE, Bonow RO, Arce J. Noninvasive assessment of left ventricular diastolic function by pulsed Doppler echocardiography in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 1987; 10:733–742.
Article29. Maron BJ, Spirito P. Implications of left ventricular remodeling in hypertrophic cardiomyopathy. Am J Cardiol. 1998; 81:1339–1344.30. Spirito P, Maron BJ, Bonow RO, Epstein SE. Occurrence and significance of progressive left ventricular wall thinning and relative cavity dilatation in hypertrophic cardiomyopathy. Am J Cardiol. 1987; 60:123–129.
Article31. Hina K, Kusachi S, Iwasaki K, Nogami K, Moritani H, Kita T, et al. Progression of left ventricular enlargement in patients with hypertrophic cardiomyopathy: incidence and prognostic value. Clin Cardiol. 1993; 16:403–407.
Article32. Tsunakawa H, Wei D, Mashima S, Harumi K. Study on the genesis of giant negative T wave in apical hypertrophic cardiomyopathy using a three-dimensional computer model. Jpn Heart J. 1991; 32:799–809.
Article33. Rowin EJ, Maron BJ, Appelbaum E, Link MS, Gibson CM, Lesser JR, et al. Significance of false negative electrocardiograms in preparticipation screening of athletes for hypertrophic cardiomyopathy. Am J Cardiol. 2012; 110:1027–1032.
Article34. Lakdawala NK, Thune JJ, Maron BJ, Cirino AL, Havndrup O, Bundgaard H, et al. Electrocardiographic features of sarcomere mutation carriers with and without clinically overt hypertrophic cardiomyopathy. Am J Cardiol. 2011; 108:1606–1613.
Article35. Park SY, Park TH, Kim JH, Baek HK, Seo JM, Kim WJ, et al. Relationship between giant negative T-wave and severity of apical hypertrophy in patients with apical hypertrophic cardiomyopathy. Echocardiography. 2010; 27:770–776.
Article36. Tikkanen JT, Anttonen O, Junttila MJ, Aro AL, Kerola T, Rissanen HA, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009; 361:2529–2537.
Article37. Jeong JH. Prevalence of and risk factors for atrial fibrillation in Korean adults older than 40 years. J Korean Med Sci. 2005; 20:26–30.
Article38. Iguchi Y, Kimura K, Aoki J, Kobayashi K, Terasawa Y, Sakai K, et al. Prevalence of atrial fibrillation in community-dwelling Japanese aged 40 years or older in Japan: analysis of 41,436 non-employee residents in Kurashiki-city. Circ J. 2008; 72:909–913.
Article39. Lok NS, Lau CP. Prevalence of palpitations, cardiac arrhythmias and their associated risk factors in ambulant elderly. Int J Cardiol. 1996; 54:231–236.
Article40. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001; 285:2370–2375.
Article41. Olivotto I, Cecchi F, Casey SA, Dolara A, Traverse JH, Maron BJ. Impact of atrial fibrillation on the clinical course of hypertrophic cardiomyopathy. Circulation. 2001; 104:2517–2524.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-invasive Assessment of Hypertrophic Cardiomyopathy
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
- Tips for Successful Septal Myectomy in Patients with Hypertrophic Cardiomyopathy
- A Case of Dexamethasone induced Hypertrophic Cardiomyopathy in Neonate with Bronchopulmonary Dysplasia
- A Case of Regressed Apical Hypertrophic Cardiomyopathy
