Korean J Ophthalmol.
2014 Dec;28(6):431-435. 10.3341/kjo.2014.28.6.431.
Levator Resection in the Management of Myopathic Ptosis
- Affiliations
-
- 1Eye Clinic, Haydarpasa Numune Education and Research Hospital, Istanbul, Turkey. bulent_but@yahoo.com
- KMID: 2345818
- DOI: http://doi.org/10.3341/kjo.2014.28.6.431
Abstract
- PURPOSE
To evaluate the results of levator resection in patients with myopathic ptosis.
METHODS
The medical records of consecutive patients who underwent levator resection surgery performed for myopathic ptosis between October 2009 and March 2013 were reviewed. Indications for surgery were ptosis obscuring the visual axis and margin-reflex distance < or =2 mm. Surgical success was defined as clear pupillary axis when the patient voluntarily opened his eye and margin-reflex distance > or =3 mm. We analyzed the effect of levator function and Bell's phenomenon on the rates of success and corneal complication.
RESULTS
This series included six male and six female patients. Levator function was between 4 and 12 mm. We performed bilateral levator resection surgery in all patients. The mean follow-up time was 14.8 months (range, 6 to 36 months). No patient was overcorrected. Adequate lid elevation was achieved after the operation in 20 eyes. Ptosis recurred in three out of 20 eyes after adequate lid elevation was achieved. Our overall success rate was 70.8%. In three eyes with poor Bell's phenomenon, corneal irritation and punctate epitheliopathy that required artificial eye drops and ointments developed in the early postoperative period, although symptoms resolved completely within 2 months of the resection surgery. No patients required levator recession or any other revision surgery for lagophthalmos or corneal exposure after levator resection.
CONCLUSIONS
Levator resection seems to be a safe and effective procedure in myopathic patients with moderate or good Bell's phenomenon and levator function greater than 5 mm.
Keyword
MeSH Terms
Figure
-

Fig. 1 A myotonic-dystrophy patient with myopathic ptosis.
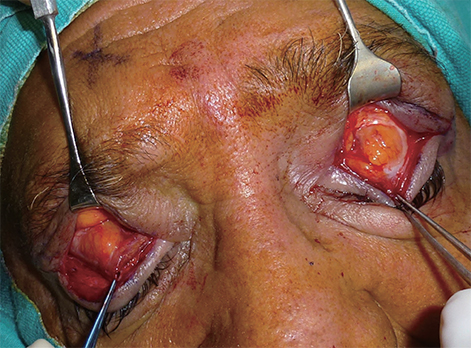
Fig. 2 Fat infiltration of levator muscles.

Fig. 3 Early postoperative period of the same patient. Pupillary axis is clear and no sign of corneal exposure is present
Reference
-
1. Ahn J, Kim NJ, Choung HK, et al. Frontalis sling operation using silicone rod for the correction of ptosis in chronic progressive external ophthalmoplegia. Br J Ophthalmol. 2008; 92:1685–1688.2. Kearns TP, Sayre GP. Retinitis pigmentosa, external ophthalmophegia, and complete heart block: unusual syndrome with histologic study in one of two cases. AMA Arch Ophthalmol. 1958; 60:280–289.3. Fang W, Huang CC, Lee CC, et al. Ophthalmologic manifestations in MELAS syndrome. Arch Neurol. 1993; 50:977–980.4. Burian HM, Burns CA. Ocular changes in myotonic dystrophy. Am J Ophthalmol. 1967; 63:22–34.5. Wong VA, Beckingsale PS, Oley CA, Sullivan TJ. Management of myogenic ptosis. Ophthalmology. 2002; 109:1023–1031.6. Soejima K, Sakurai H, Nozaki M, et al. Surgical treatment of blepharoptosis caused by chronic progressive external ophthalmoplegia. Ann Plast Surg. 2006; 56:439–442.7. Bernardini FP, de Conciliis C, Devoto MH. Frontalis suspension sling using a silicone rod in patients affected by myogenic blepharoptosis. Orbit. 2002; 21:195–198.8. Roefs AM, Waters PJ, Moore GR, Dolman PJ. Orbicularis oculi muscle biopsies for mitochondrial DNA analysis in suspected mitochondrial myopathy. Br J Ophthalmol. 2012; 96:1296–1299.9. Taylor RW, Turnbull DM. Mitochondrial DNA mutations in human disease. Nat Rev Genet. 2005; 6:389–402.10. Buttanri IB, Serin D, Karslioglu S, et al. Effect of suturing the silicone rod to the tarsal plate and the suture material used on success of frontalis suspension surgery. Ophthal Plast Reconstr Surg. 2013; 29:98–100.11. Collin JR. A manual of systematic eyelid surgery. Edinburgh: Churchill Livingstone;1983. p. 44–64.12. Kemp EG, James CR, Collin JRO. Brow suspension in the management of ptosis: an analysis of over 100 cases. Trans Ophthalmol Soc U K. 1986; 105:84–87.13. Lane CM, Collin JR. Treatment of ptosis in chronic progressive external ophthalmoplegia. Br J Ophthalmol. 1987; 71:290–294.14. Rodrigue D, Molgat YM. Surgical correction of blepharoptosis in oculopharyngeal muscular dystrophy. Neuromuscul Disord. 1997; 7:Suppl 1. S82–S84.15. Leibovitch I, Leibovitch L, Dray JP. Long-term results of frontalis suspension using autogenous fascia lata for congenital ptosis in children under 3 years of age. Am J Ophthalmol. 2003; 136:866–871.16. Liu D. Blepharoptosis correction with frontalis suspension using a supramid sling: duration of effect. Am J Ophthalmol. 1999; 128:772–773.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation of Congenital Blepharoptosis
- Outcomes of Anterior Levator Resection and Frontalis Sling in Congenital Ptosis with Poor Levator Function
- Clinical Study of Simple Levator Resection in Ptosis Patients
- Eyelid Blink Characteristics in Patients with Ptosis Assessed Using Cellphone Camera before and after Levator Resection
- External Levator Resection in Mild to Moderate Unilateral Ptosis
