Isolated Mass-Forming IgG4-Related Cholangitis as an Initial Clinical Presentation of Systemic IgG4-Related Disease
- Affiliations
-
- 1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kt12.jang@samsung.com
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2345553
- DOI: http://doi.org/10.4132/jptm.2015.12.01
Abstract
- IgG4-related disease (IgG4-RD) may involve multiple organs. Although it usually presents as diffuse organ involvement, localized mass-forming lesions have been occasionally encountered in pancreas. However, the same pattern has been seldom reported in biliary tract. A 61-year-old male showed a hilar bile duct mass with multiple enlarged lymph nodes in imaging studies and he underwent trisectionectomy under impression of cholangiocarcinoma. Gross examination revealed a mass-like lesion around hilar bile duct. Histopathologically, dense lymphoplasmacytic infiltration and storiform fibrosis were identified without evidence of malignancy. Immunohistochemical stain demonstrated rich IgG4-positive plasma cell infiltration. Follow-up imaging studies disclosed multiple enlarged lymph nodes with involvement of pancreas and perisplenic soft tissue. The lesions have been significantly reduced after steroid treatment, which suggests multi-organ involvement of systemic IgG4-RD. Here, we report an unusual localized mass-forming IgG4-related cholangitis as an initial presentation of IgG4-RD, which was biliary manifestation of systemic IgG4-related autoimmune disease.
MeSH Terms
Figure
-

Fig. 1. Magnetic resonance imaging reveals an enhancing mass lesion which has high signal intensity on diffusion restriction phase (A) and low intensity on apparent diffusion coefficient map phase (B), suspicious for malignancy. (C) The cut section of hilar bile duct shows a relatively well-demarcated mass-forming lesion with a hepatic parenchymal invasion.
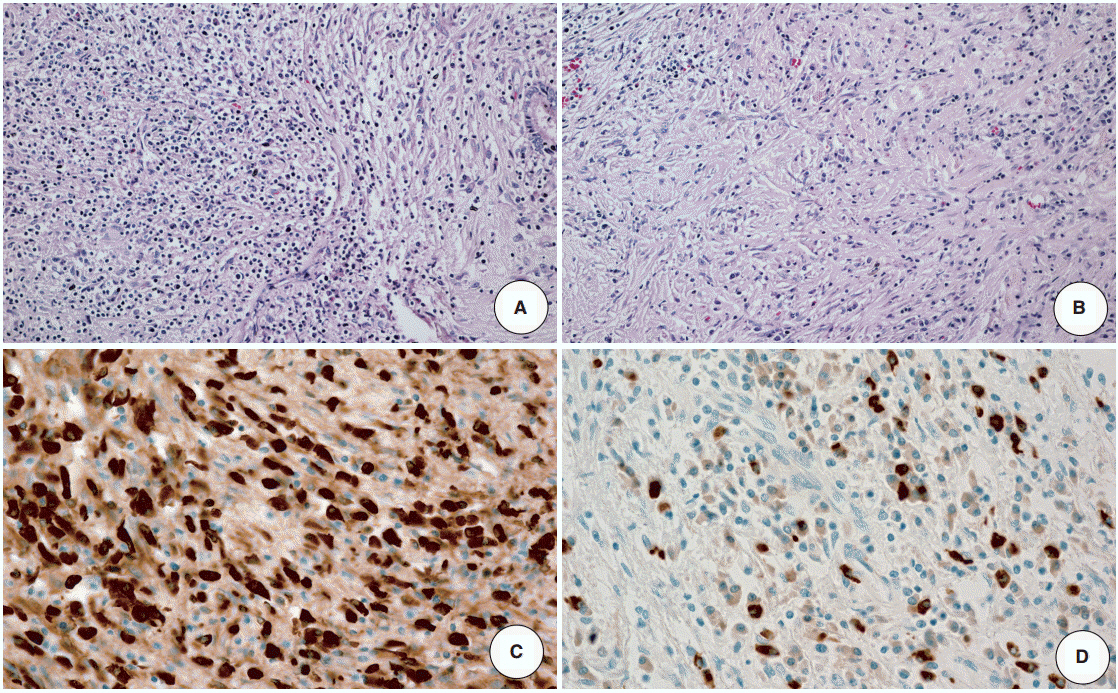
Fig. 2. Histologic examination reveals dense infiltration of lymphocytes and plasma cells (A) and storiform fibrosis (B). Both IgG-immunopositive (C) and IgG4-immunopositive (D) plasma cells are identified by immunohistochemical staining.

Fig. 3. (A) Fluorodeoxyglucose (FDG) positron emission tomography–computed tomography, maximum intensity projection image show hypermetabolic lesions involving bilateral supraclavicular, left axillar, mediastinal, pulmonary hilar and retroperitoneal lymph nodes, right liver biliary tract, pancreas, and perisplenic area. (B) After steroid treatment, markedly decreased FDG uptake is noted although uptakes in some lymph nodes are still seen.
Cited by 1 articles
-
Pathologic interpretation of endoscopic ultrasound–guided fine needle aspiration cytology/biopsy for pancreatic lesions
Haeryoung Kim, Kee-Taek Jang
J Pathol Transl Med. 2020;54(5):367-377. doi: 10.4132/jptm.2020.07.21.
Reference
-
1. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010; 34:1812–9.2. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–92.3. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–51.
Article4. Mahajan VS, Mattoo H, Deshpande V, Pillai SS, Stone JH. IgG4-related disease. Annu Rev Pathol. 2014; 9:315–47.
Article5. Chang WI, Kim BJ, Lee JK, et al. The clinical and radiological characteristics of focal mass-forming autoimmune pancreatitis: comparison with chronic pancreatitis and pancreatic cancer. Pancreas. 2009; 38:401–8.6. Matsumoto I, Shinzeki M, Toyama H, et al. A focal mass-forming autoimmune pancreatitis mimicking pancreatic cancer with obstruction of the main pancreatic duct. J Gastrointest Surg. 2011; 15:2296–8.
Article7. Naitoh I, Nakazawa T, Hayashi K, et al. Clinical differences between mass-forming autoimmune pancreatitis and pancreatic cancer. Scand J Gastroenterol. 2012; 47:607–13.
Article8. Deshpande V, Sainani NI, Chung RT, et al. IgG4-associated cholangitis: a comparative histological and immunophenotypic study with primary sclerosing cholangitis on liver biopsy material. Mod Pathol. 2009; 22:1287–95.
Article9. Zen Y, Harada K, Sasaki M, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol. 2004; 28:1193–203.10. Hamano H, Kawa S, Uehara T, et al. Immunoglobulin G4-related lymphoplasmacytic sclerosing cholangitis that mimics infiltrating hilar cholangiocarcinoma: part of a spectrum of autoimmune pancreatitis? Gastrointest Endosc. 2005; 62:152–7.
Article11. Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–8.
Article12. Kawano M, Saeki T, Nakashima H, et al. Proposal for diagnostic criteria for IgG4-related kidney disease. Clin Exp Nephrol. 2011; 15:615–26.
Article13. Novotný I, Dítě P, Trna J, Lata J, Husová L, Geryk E. Immunoglobulin G4-related cholangitis: a variant of IgG4-related systemic disease. Dig Dis. 2012; 30:216–9.
Article14. Deshpande V. IgG4-related disease of the gastrointestinal tract: a 21st century chameleon. Arch Pathol Lab Med. 2015; 139:742–9.
Article15. Miki A, Sakuma Y, Ohzawa H, et al. Immunoglobulin g4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma diagnosed with following bile duct resection: report of a case. Int Surg. 2015; 100:480–5.
Article16. Graham RP, Smyrk TC, Chari ST, Takahashi N, Zhang L. Isolated IgG4-related sclerosing cholangitis: a report of 9 cases. Hum Pathol. 2014; 45:1722–9.
Article17. Cheuk W, Yuen HK, Chu SY, Chiu EK, Lam LK, Chan JK. Lymphadenopathy of IgG4-related sclerosing disease. Am J Surg Pathol. 2008; 32:671–81.
Article18. Ohara H, Okazaki K, Tsubouchi H, et al. Clinical diagnostic criteria of IgG4-related sclerosing cholangitis 2012. J Hepatobiliary Pancreat Sci. 2012; 19:536–42.19. Lazaridis KN. Sclerosing cholangitis epidemiology and etiology. J Gastrointest Surg. 2008; 12:417–9.
Article20. Chung DT, Tang CN, Lai EC, Yang GP, Li MK. Immunoglobulin G4-associated sclerosing cholangitis mimicking cholangiocarcinoma. Hong Kong Med J. 2010; 16:149–52.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunoglobulin G4-related sclerosing cholangitis
- Advances in IgG4-related Hepatobiliary Disease
- Classification and Diagnostic Criteria for IgG4-Related Sclerosing Cholangitis
- Recent Updates of Immunoglobulin G4-related Pancreatobiliary Disease
- Role of Endoscopic Procedures in the Diagnosis of IgG4-Related Pancreatobiliary Disease
