Preservation of Internal Iliac Artery after Endovascular Repair of Common Iliac Artery Dissection Using Modified Fenestrated Stent Graft
- Affiliations
-
- 1Department of Vascular Surgery, First Affiliated Hospital of Anhui Medical University, Hefei, China. huagzhu@yeah.net
- KMID: 2344455
- DOI: http://doi.org/10.4070/kcj.2016.46.3.412
Abstract
- Standard endovascular repair of iliac/aortoiliac pathologies can lead to complications, such as buttock claudication, colon ischemia and erectile dysfunction. Branch grafts have been developed but require at least 6 weeks for customization and are not currently available in China; they are also quite expensive. To our knowledge, modified fenestrated stent grafts (MFSGs) are a safe and effective alternative for treating patients with juxtarenal aneurysms. Most MFSGs are used for the preservation of renal and left subclavian arteries. Few cases of MFSGs have been reported in the treatment of iliac pathologies. The use of an MFSG is decided on a case-by-case basis. This report presents our first clinical use of an MFSG for preservation of the internal iliac artery.
Keyword
MeSH Terms
Figure
-

Fig. 1 Three-dimensional reconstructed images show a slightly dilated common iliac artery (CIA), as well as dissection from the CIA to the external iliac artery with intimal tears in the CIA, without dilation of the internal iliac artery.

Fig. 2 An ophthalmologic cautery was used to carefully burn the Dacron fabric to create the fenestration.

Fig. 3 A longitudinal radiopaque marker was sutured to the polyester graft for orientation just below the fenestrated ostium using 6-0 Prolene sutures.

Fig. 4 The aortogram revealed right iliac dissection with intimal tears in the common iliac artery, which was limited to the proximal end of the external iliac artery at the left anterior oblique 40°+caudal 15° projection angle.
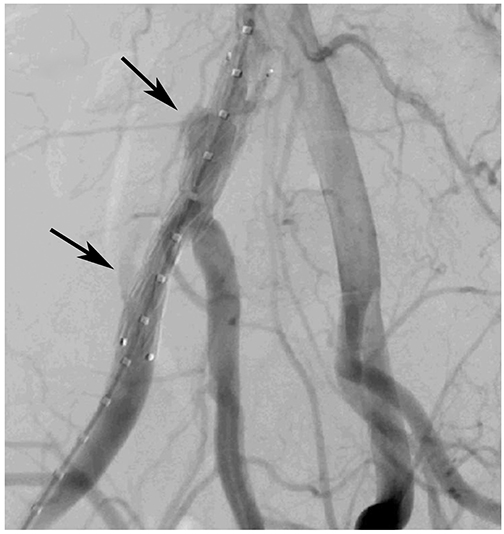
Fig. 5 The aortogram revealed that the iliac dissection successfully excluded and preserved the flow of the internal iliac artery. Arrows show the endoleak Ib (down) and IV (up).
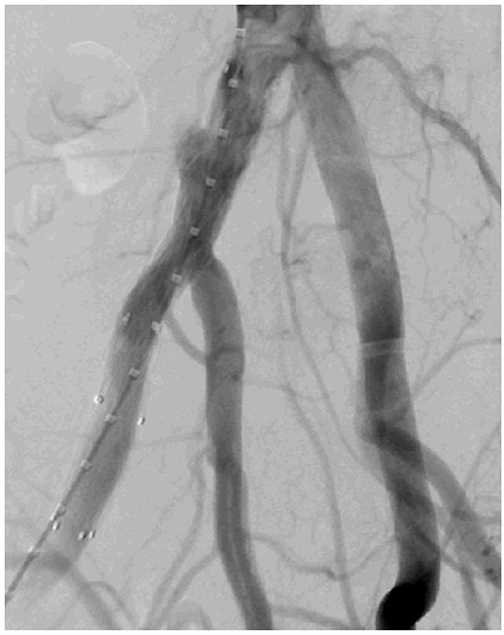
Fig. 6 Repeat angiography showed intact flow into the internal iliac artery, a narrowed endoleak IV, and the disappearance of endoleak Ib.
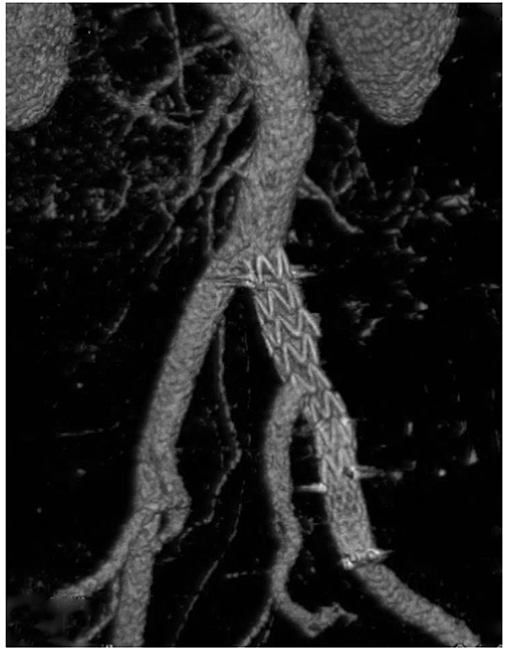
Fig. 7 Three-dimensional reconstructed images after 5 months revealed no endoleaks and showed a patent right internal iliac artery. The preplanned fenestration was closely aligned with the vessel ostia.
Reference
-
1. Kwak HS, Han YM, Chung GH, Yu HC, Jeong YJ. Isolated spontaneous dissection of the common iliac artery: percutaneous stent placement in two patients. Cardiovasc Intervent Radiol. 2006; 29:883–885.2. Farahmand P, Becquemin JP, Desgranges P, Allaire E, Marzelle J, Roudot-Thoraval F. Is hypogastric artery embolization during endovascular aortoiliac aneurysm repair (EVAR) innocuous and useful? Eur J Vasc Endovasc Surg. 2008; 35:429–435.3. Parlani G, Verzini F, De Rango P, et al. Long-term results of iliac aneurysm repair with iliac branched endograft: a 5-year experience on 100 consecutive cases. Eur J Vasc Endovasc Surg. 2012; 43:287–292.4. Oderich GS, Ricotta JJ 2nd. Novel surgeon-modified hypogastric branch stent graft to preserve pelvic perfusion. Ann Vasc Surg. 2010; 24:278–286.5. Honjo O, Yamada Y, Kuroko Y, Kushida Y, Une D, Hioki K. Spontaneous dissection and rupture of common iliac artery in a patient with fibromuscular dysplasia: a case report and review of the literature on iliac artery dissections secondary to fibromuscular dysplasia. J Vasc Surg. 2004; 40:1032–1036.6. Cook PS, Erdoes LS, Selzer PM, Rivera FJ, Palmaz JC. Dissection of the external iliac artery in highly trained athletes. J Vasc Surg. 1995; 22:173–177.7. Kwon SH, Oh JH. Successful interventional treatment of a spontaneous right common iliac artery dissection extending retrogradely into the left external iliac artery. J Vasc Interv Radiol. 2006; 17:717–721.8. Stone PA, Campbell JE, Hass SM, Jain A, Kazmi H. Kissing iliac artery stent technique for salvage of hypogastric artery occlusion secondary to iliac artery dissection during endovascular aneurysm repair. Vasc Endovascular Surg. 2011; 45:174–177.9. Lee CW, Kaufman JA, Fan CM, et al. Clinical outcome of internal iliac artery occlusions during endovascular treatment of aortoiliac aneurysmal diseases. J Vasc Interv Radiol. 2000; 11:567–571.10. Oderich GS, Ricotta JJ 2nd. Modified fenestrated stent grafts: device design, modifications, implantation, and current applications. Perspect Vasc Surg Endovasc Ther. 2009; 21:157–167.11. Ricotta JJ 2nd, Tsilimparis N. Surgeon-modified fenestratedbranched stent grafts to treat emergently ruptured and symptomatic complex aortic aneurysms in high-risk patients. J Vasc Surg. 2012; 56:1535–1542.12. Starnes BW. Physician-modified endovascular grafts for the treatment of elective, symptomatic, or ruptured juxtarenal aortic aneurysms. J Vasc Surg. 2012; 56:601–607.13. Redlinger RE Jr, Ahanchi SS, Panneton JM. In situ laser fenestration during emergent thoracic endovascular aortic repair is an effective method for left subclavian artery revascularization. J Vasc Surg. 2013; 58:1171–1177.14. Naughton PA, Park MS, Kheirelseid EA, et al. A comparative study of the bell-bottom technique vs hypogastric exclusion for the treatment of aneurysmal extension to the iliac bifurcation. J Vasc Surg. 2012; 55:956–962.15. Lobato AC, Camacho-Lobato L. The sandwich technique to treat complex aortoiliac or isolated iliac aneurysms: results of midterm follow-up. J Vasc Surg. 2013; 57:2 Suppl. 26S–34S.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Novel Strategies for the Hostile Iliac Artery during Endovascular Aortic Aneurysm Repair
- Endovascular aortic aneurysm repair using a bifurcated stent graft in a patient with femoro-femoral bypass
- Endovascular Treatment of Isolated Bilateral Common Iliac Artery Aneurysms Using Iliac Branched Stent Graft
- Endovascular Repair of an Iliac Artery Pseudoaneurysm Using a Surgeon-Reconstructed Prosthetic Graft and a Bare Metal Stent
