Higher Blood Pressure Variability in White Coat Hypertension; from the Korean Ambulatory Blood Pressure Monitoring Registry
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Ewha Womans University, Seoul, Korea. pwb423@ewha.ac.kr
- 2Department of Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea.
- 3Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 4Department of Internal Medicine, School of Medicine, Chonnam University, Gwangju, Korea.
- 5Department of Internal Medicine, School of Medicine, Yonsei University, Seoul, Korea.
- 6Department of Internal Medicine, School of Medicine, Seoul National University, Seongnam, Korea.
- 7Department of Internal Medicine, School of Medicine Kyung Hee University, Seoul, Korea.
- KMID: 2344449
- DOI: http://doi.org/10.4070/kcj.2016.46.3.365
Abstract
- BACKGROUND AND OBJECTIVES
Blood pressure variability (BPV) was recently shown to be a risk factor of stroke. White coat hypertension (WCH) used to be regarded as innocuous, but one long-term follow-up study reported that WCH increased stroke rate compared to normotension (NT). In this study, we aimed to evaluate the relationship between WCH and BPV.
SUBJECTS AND METHODS
We analyzed 1398 subjects from the Korean Ambulatory Blood Pressure Registry, who were divided into NT (n=364), masked hypertension (n=122), white coat hypertension (n=254), and sustained hypertension (n=658) groups.
RESULTS
Baseline characteristics were similar among groups. The average real variability (ARV), a highly sensitive BPV parameter, was highest in the WCH group, followed by the sustained hypertension, masked hypertension, and NT groups. The results persisted after being adjusted for covariates. The WCH vs. sustained hypertension results (adjusted mean±standard error) were as follows: 24-h systolic ARV, 22.9±0.8 vs. 19.4±0.6; 24-h diastolic ARV, 16.8±0.6 vs. 14.3±0.5; daytime systolic ARV, 21.8±0.8 vs. 16.8±0.6; and daytime diastolic ARV, 16.2±0.6 vs. 13.4±0.5 (p<0.001 for all comparisons).
CONCLUSION
From the registry data, we found that subjects with WCH or masked hypertension had higher BPV than NT. However, long-term follow-up data assessing the clinical influences of WCH on stroke are needed.
MeSH Terms
Figure
-

Fig. 1 Flow chart of study population. Kor-ABP: Korean ambulatory blood pressure, BP: blood pressure.
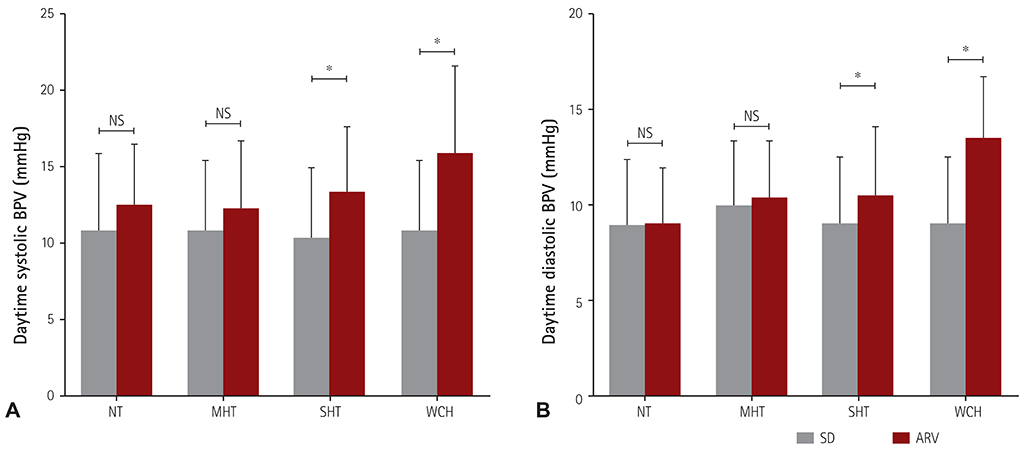
Fig. 2 The differences between SD and ARV within groups. The WCH group showed a large difference in the SD and ARV, which was followed by SHT. The NT and MHT groups did not show differences in daytime systolic BPV (A) or daytime diastolic BPV (B). *p<0.001. SD: standard deviation, ARV: average real variability, WCH: white coat hypertension, SHT: sustained hypertension, NT: normotension, MHT: masked hypertension, BPV: blood pressure variability, NS: non-significant.
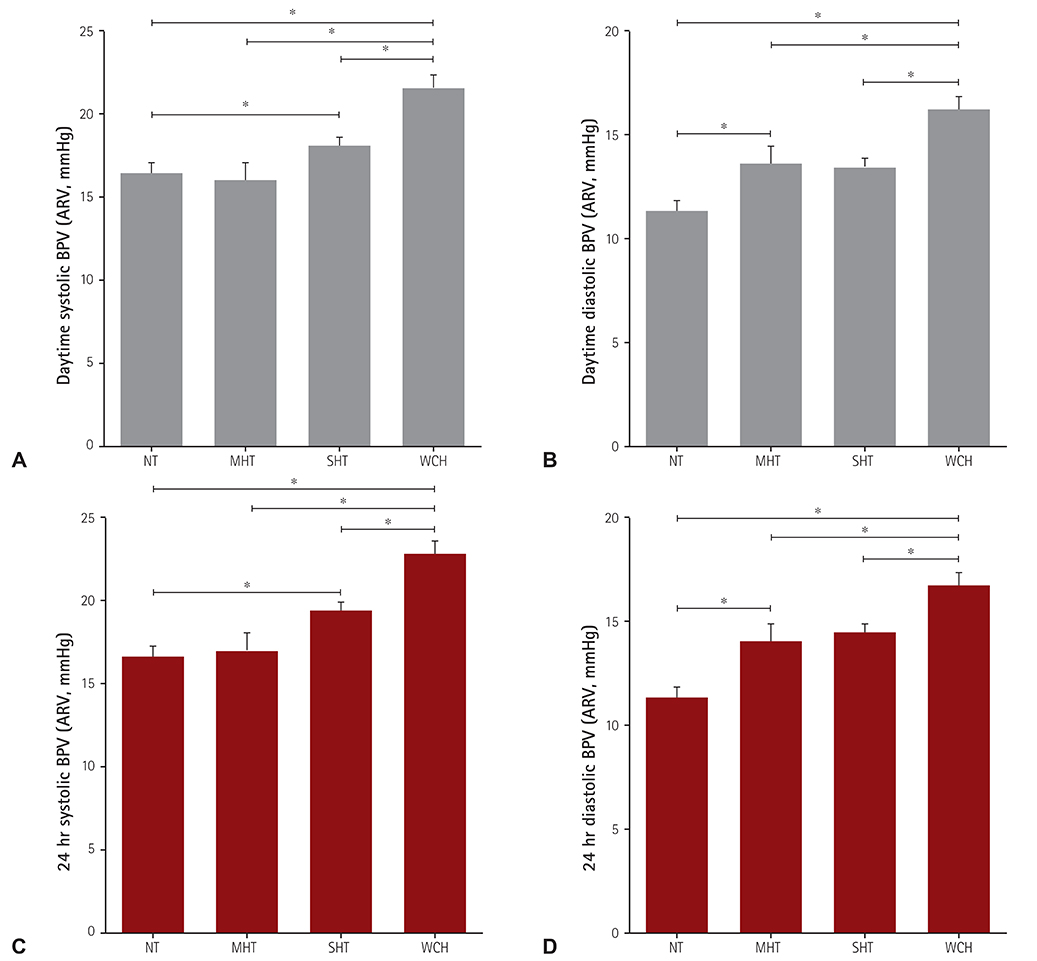
Fig. 3 The difference in ARV between groups. The WCH group shows the highest value of ARV compared to the other three groups. ARV values represent means adjusted for sex, age, diabetes mellitus, body mass index, serum creatinine, and cholesterol level. (A) Daytime SBP ARV, (B) daytime DBP ARV, (C) 24-hour SBP ARV, (D) 24-hour DBP ARV. *p<0.001. ARV: average real variability, WCH: white coat hypertension, SBP: systolic blood pressure, DBP: diastolic blood pressure, BPV: blood pressure variability, NT: normotension, MHT: masked hypertension, SHT: sustained hypertension.
Reference
-
1. Julius S, Mejia A, Jones K, et al. "White coat" versus "sustained" borderline hypertension in Tecumseh, Michigan. Hypertension. 1990; 16:617–623.2. Verdecchia P, Schillaci G, Boldrini F, Zampi I, Porcellati C. Variability between current definitions of 'normal' ambulatory blood pressure. Implications in the assessment of white coat hypertension. Hypertension. 1992; 20:555–562.3. Bonow RO, Mann DL, Zipes DP, Libby P. Braunwald's Heart Disease. 9th ed. Philadelphia: Elsevier Health Sciences;2012. p. 218.4. Fagard RH, Cornelissen VA. Incidence of cardiovascular events in white-coat, masked and sustained hypertension versus true normotension: a meta-analysis. J Hypertens. 2007; 25:2193–2198.5. Ohkubo T, Kikuya M, Metoki H, et al. Prognosis of "masked" hypertension and "white-coat" hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol. 2005; 46:508–515.6. Mancia G, Bombelli M, Brambilla G, et al. Long-term prognostic value of white coat hypertension: an insight from diagnostic use of both ambulatory and home blood pressure measurements. Hypertension. 2013; 62:168–174.7. Glen SK, Elliott HL, Curzio JL, Lees KR, Reid JL. White-coat hypertension as a cause of cardiovascular dysfunction. Lancet. 1996; 348:654–657.8. Mancia G, Facchetti R, Bombelli M, Grassi G, Sega R. Long-term risk of mortality associated with selective and combined elevation in office, home, and ambulatory blood pressure. Hypertension. 2006; 47:846–853.9. Rothwell PM. Limitations of the usual blood-pressure hypothesis and importance of variability, instability, and episodic hypertension. Lancet. 2010; 375:938–948.10. Pierdomenico SD, Di Nicola M, Esposito AL, et al. Prognostic value of different indices of blood pressure variability in hypertensive patients. Am J Hypertens. 2009; 22:842–847.11. Rothwell PM, Howard SC, Dolan E, et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010; 375:895–905.12. Poortvliet RK, Ford I, Lloyd SM, et al. Blood pressure variability and cardiovascular risk in the PROspective Study of Pravastatin in the Elderly at Risk (PROSPER). PLoS One. 2012; 7:e52438.13. Endo K, Kario K, Koga M, et al. Impact of early blood pressure variability on stroke outcomes after thrombolysis: the SAMURAI rt-PA Registry. Stroke. 2013; 44:816–818.14. Schillaci G, Bilo G, Pucci G, et al. Relationship between short-term blood pressure variability and large-artery stiffness in human hypertension: findings from 2 large databases. Hypertension. 2012; 60:369–377.15. Zakopoulos NA, Tsivgoulis G, Barlas G, et al. Impact of the time rate of blood pressure variation on left ventricular mass. J Hypertens. 2006; 24:2071–2077.16. Franks PW. White-coat hypertension and risk of stroke: do the data really tell us what we need to know? Hypertension. 2005; 45:183–184.17. Kang IS, Pyun WB, Shin J, Kim JH, Kim SG, Shin GJ. Association between central obesity and circadian parameters of blood pressure from the korean ambulatory blood pressure monitoring registry: Kor-ABP registry. J Korean Med Sci. 2013; 28:1461–1467.18. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003; 42:1206–1252.19. Mena L, Pintos S, Queipo NV, Aizpúrua JA, Maestre G, Sulbarán T. A reliable index for the prognostic significance of blood pressure variability. J Hypertens. 2005; 23:505–511.20. Cacciolati C, Tzourio C, Hanon O. Blood pressure variability in elderly persons with white-coat and masked hypertension compared to those with normotension and sustained hypertension. Am J Hypertens. 2013; 26:367–372.21. Myers MG. Pseudoresistant hypertension attributed to white-coat effect. Hypertension. 2012; 59:532–533.22. Björklund K, Lind L, Vessby B, Andrén B, Lithell H. Different metabolic predictors of white-coat and sustained hypertension over a 20-year follow-up period: a population-based study of elderly men. Circulation. 2002; 106:63–68.23. Sorof JM, Poffenbarger T, Franco K, Portman R. Evaluation of white coat hypertension in children: importance of the definitions of normal ambulatory blood pressure and the severity of casual hypertension. Am J Hypertens. 2001; 14(9 Pt 1):855–860.24. Parati G, Di Rienzo M, Mancia G. Neural cardiovascular regulation and 24-hour blood pressure and heart rate variability. Ann N Y Acad Sci. 1996; 783:47–63.25. Pickering TG. Variability of blood pressure. Blood Press Monit. 1998; 3:141–145.26. Diaz KM, Veerabhadrappa P, Kashem MA, et al. Relationship of visit-to-visit and ambulatory blood pressure variability to vascular function in African Americans. Hypertens Res. 2012; 35:55–61.27. Verdecchia P, Reboldi GP, Angeli F, et al. Short- and long-term incidence of stroke in white-coat hypertension. Hypertension. 2005; 45:203–208.28. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013; 34:2159–2219.29. Hong KS, Bang OY, Kang DW, et al. Stroke statistics in Korea: part I. Epidemiology and risk factors: a report from the korean stroke society and clinical research center for stroke. J Stroke. 2013; 15:2–20.30. Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015; 131:434–441.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Comparison of White Coat Effect in Elderly White Coat Hypertensive Patients with Youngers
- Clinical Usefulness of 24-hour Ambulatory Blood Pressure Monitoring in Hypertensive Pregnancy
- Clinical Significance of Nighttime Blood Pressure
- Role of ambulatory blood pressure monitoring in elderly hypertensive patients
- Clinical Manifestation of Ambulatory Blood Pressure Monitoring in Children and Adolescent with Hypertension
