Breast reconstruction using implants
- Affiliations
-
- 1Department of Plastic Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea School of Medicine, Seoul, Korea. stahn@catholic.ac.kr
Abstract
- Since the early detection rate of breast cancer is increasing and skin- or nipple-sparing mastectomies have become popularized recently, the need for breast reconstruction using implants is continuously increasing. Simplicity of surgical techniques, short operation time, short hospital stay, short recovery time, no need for donor site defects and scars, and reconstruction with tissue of same color, texture, and sensation are the main advantages of implant reconstruction. However, reconstructed breasts using implants tend to be less natural and ptotic, sensitive to external temperature, unable to adapt to the normal aging process of the breast, and may have implant related complications. In patients with postoperative radiation, implant reconstruction is not indicated because of decreased skin flap circulation and increased implant related complications. Although autologous tissue reconstruction is known to produce natural and aesthetic breasts, similar results can be achieved by implant reconstruction when it is well indicated and performed with appropriate techniques by experienced surgeons. Implant reconstruction is best suited for young, active women with small round breasts and slender bodies.
MeSH Terms
Figure
-
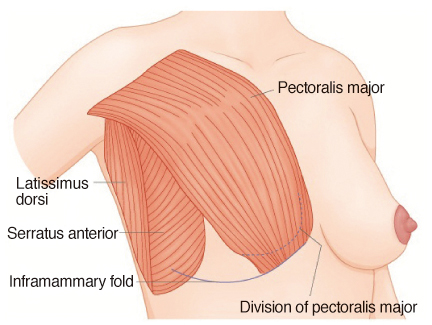
Figure 1 Pocket design for expander/implant insertion. The inferomedial insertion of pectoralis major muscle is cut to relieve tension and unwanted muscle action around the implant (From Ahn ST. Aesthetic and reconstructive breast surgery. Seoul: Koonja Publishing Co.; 2010, with permission from Koonja Publishing Co.) [13].
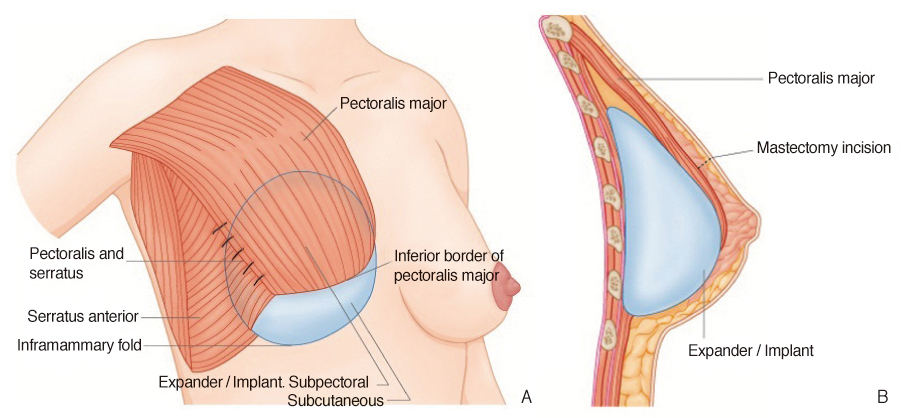
Figure 2 Expander/implant insertion. (A) The lateral margin of the pectoralis major muscle is sutured to the serratus anterior muscle flap. The upper part of the implant is covered by the pectoralis major muscle and lower part is in the subcutaneous position. (B) Lateral view after implant insertion. The skin incision is located over the pectoralis major muscle (From Ahn ST. Aesthetic and reconstructive breast surgery. Seoul: Koonja Publishing Co.; 2010, with permission from Koonja Publishing Co.) [13].
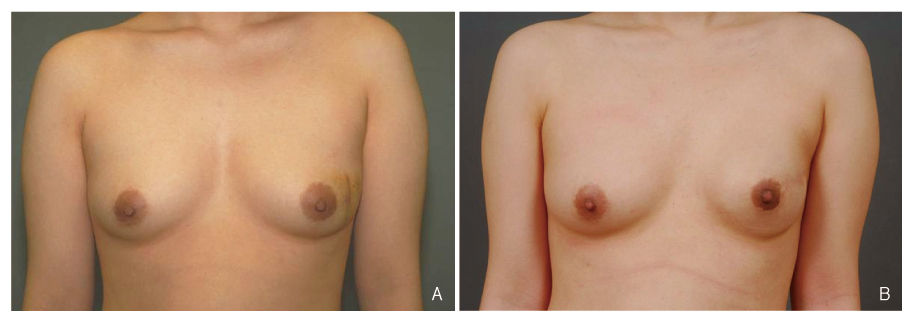
Figure 3 Immediate breast reconstruction using an implant only in the patient with the nipple sparing mastectomy. (A) Preoperative view. (B) Postoperative view after reconstruction with a 250 mL implant.
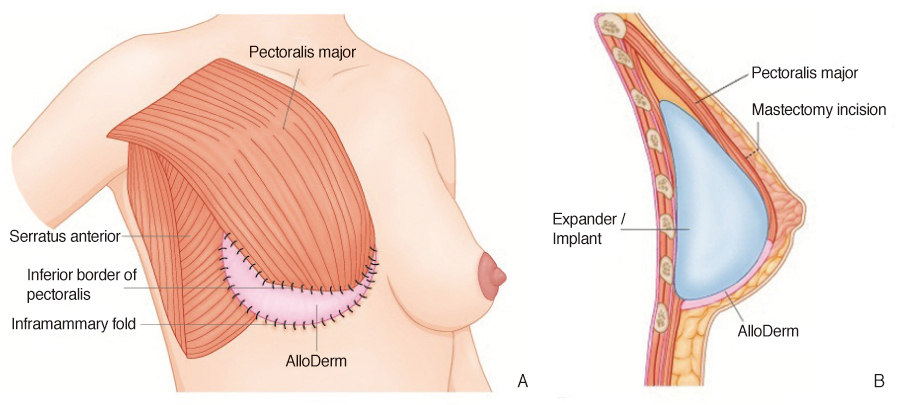
Figure 4 Expander/implant insertion using AlloDerm. (A) AlloDerm is sutured between the inferior margin of the pectoralis major muscle and the inframammary fold to reinforce the subcutaneous pocket. The serratus anterior muscle flap is not elevated to fix the AlloDerm. (B) AlloDerm supplemented as an additional layer between the subcutaneous pocket and implant (From Ahn ST. Aesthetic and reconstructive breast surgery. Seoul: Koonja Publishing Co.; 2010, with permission from Koonja Publishing Co.) [13].
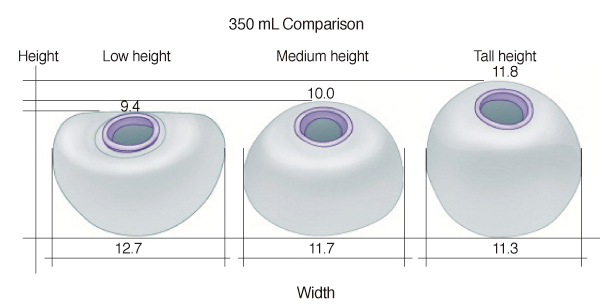
Figure 5 Siltex contour profile breast tissue expander (Mentor, Santa Barbara, CA, USA). Comparison of width and hight among low-, medium-, tall-height expanders (From Ahn ST. Aesthetic and reconstructive breast surgery. Seoul: Koonja Publishing Co.; 2010, with permission from Koonja Publishing Co.) [13].
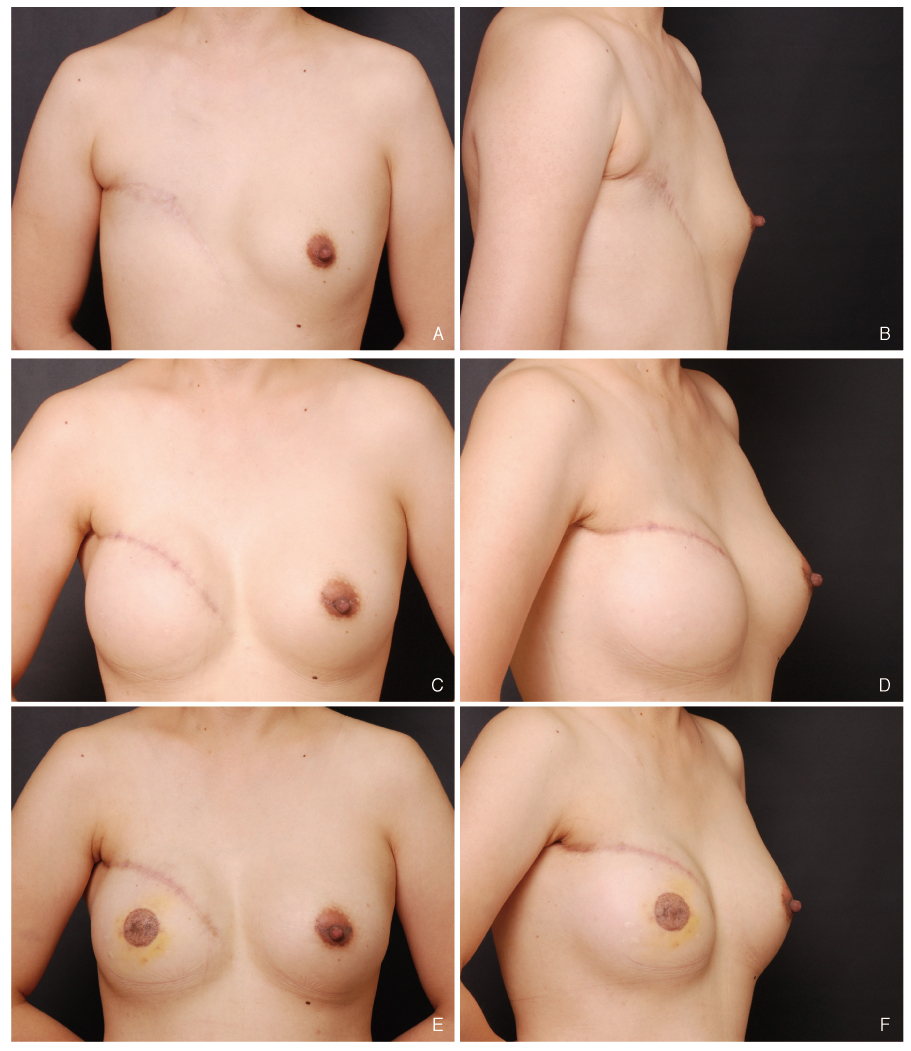
Figure 6 Delayed breast reconstruction using a tissue expander and breast implant. (A,B) Preoperative view of the 40-year-old female with the modified radical mastectomy. (C,D) Her right breast was reconstructed by 550 mL expansion with a medium-height contour profile expander and a 421 mL mid-range profile smooth cohesive silicone gel implant. Her left breast was augmented by using a 260 mL cohesive silicone gel implant. (E,F) Postoperative view after C-V flap nipple reconstruction and tattoo.
Reference
-
1. Radovan C. Breast reconstruction after mastectomy using the temporary expander. Plast Reconstr Surg. 1982. 69:195–208.
Article2. Disa JJ, McCarthy CM, Mehrara BJ, Pusic AL, Hu QY, Cordeiro PG. Postmastectomy reconstruction: an approach to patient selection. Plast Reconstr Surg. 2009. 124:43–52.
Article3. Ahn ST. Ahn ST, editor. Breast reconstruction. Aesthetic and reconstructive breast surgery. 2010. Seoul: Koonja Publishing Co.;351–376.4. NHS Information Center. Second annual report of the National Mastectomy and Breast Reconstruction Audit 2009. 2009. Leeds: NHS Information Center.5. 2009 Reconstructive surgery procedures [Internet]. 2010 Dec 9. Arlington Heights: American Society of Plastic Surgeons; http://www.plasticsurgery.org.6. Cordeiro PG, McCarthy CM. A single surgeon's 12-year experience with tissue expander/implant breast reconstruction. Part I. A prospective analysis of early complications. Plast Reconstr Surg. 2006. 118:825–831.
Article7. Cordeiro PG, McCarthy CM. A single surgeon's 12-year experience with tissue expander/implant breast reconstruction. Part II. An analysis of long-term complications, aesthetic outcomes, and patient satisfaction. Plast Reconstr Surg. 2006. 118:832–839.
Article8. Mathes SJ, Lang J. Mathes SJ, Hentz VR, editors. Breast cancer: diagnosis, therapy, and postmastectomy reconstruction. Plastic surgery. 2006. 2nd ed. Philadelphia: Elsevier;631–789.9. Nahabedian MY. Breast reconstruction: a review and rationale for patient selection. Plast Reconstr Surg. 2009. 124:55–62.
Article10. Downey S, Morales C. A survey of female plastic surgeon's attitudes toward breast reconstruction options. Plast Reconstr Surg. 2005. 116:68–69.
Article11. Sbitany H, Amalfi AN, Langstein HN. Preferences in choosing between breast reconstruction options: a survey of female plastic surgeons. Plast Reconstr Surg. 2009. 124:1781–1789.
Article12. Sigurdson L, Lalonde DH. MOC-PSSM CME article: breast reconstruction. Plast Reconstr Surg. 2008. 121:1 Suppl. 1–12.
Article13. Ahn ST. Ahn ST, editor. Breast reconstruction using implant. Aesthetic and reconstructive breast surgery. 2010. Seoul: Koonja Publishing Co.;480–490.14. Beasley ME. Spear SL. Delayed two-stage expander/implant reconstruction. Surgery of the breast: principles and art. 2006. 2nd ed. Philadelphia: Lippincott Williams and Wilkins;489–503.15. Bindingnavele V, Gaon M, Ota KS, Kulber DA, Lee DJ. Use of acellular cadaveric dermis and tissue expansion in postmastectomy breast reconstruction. J Plast Reconstr Aesthet Surg. 2007. 60:1214–1218.
Article16. Namnoum JD. Expander/implant reconstruction with AlloDerm: recent experience. Plast Reconstr Surg. 2009. 124:387–394.
Article17. Becker H. Spear SL. One-stage immediate breast reconstruction with adjustable implants. Surgery of the breast: principles and art. 2006. 2nd ed. Philadelphia: Lippincott Williams and Wilkins;438–450. .18. Eskenazi LB. New options for immediate reconstruction: achieving optimal results with adjustable implants in a single stage. Plast Reconstr Surg. 2007. 119:28–37.
Article19. Mathes SJ, Massey MF. Mathes SJ, Hentz VR. Postmastectomy reconstruction: expander-implant techniques. Plastic surgery. 2006. 2nd ed. Philadelphia: Elsevier;875–971.20. Spear SL, Pelletiere CV. Immediate breast reconstruction in two stages using textured, integrated-valve tissue expanders and breast implants. Plast Reconstr Surg. 2004. 113:2098–2103.
Article21. Strock LL. Low height tissue expanders for breast reconstruction. Innov Plast Surg. 2005. 1:71–84.22. Jones G. Decision-making: sizing and system selection. Innov Plast Surg. 2005. 1:27–38.23. Spear SL, Spittler CJ. Breast reconstruction with implants and expanders. Plast Reconstr Surg. 2001. 107:177–187.
Article24. Zienowicz RJ, Karacaoglu E. Implant-based breast reconstruction with allograft. Plast Reconstr Surg. 2007. 120:373–381.
Article25. Spear SL, Boehmler J. Spear SL. Immediate two-stage breast reconstruction using a tissue expander and implant. Surgery of the breast: principles and art. 2006. 2nd ed. Philadelphia: Lippincott Williams and Wilkins;463–483.26. Saulis AS, Mustoe TA, Fine NA. A retrospective analysis of patient satisfaction with immediate postmastectomy breast reconstruction: comparison of three common procedures. Plast Reconstr Surg. 2007. 119:1669–1676.
Article27. Spear SL, Newman MK, Bedford MS, Schwartz KA, Cohen M, Schwartz JS. A retrospective analysis of outcomes using three common methods for immediate breast reconstruction. Plast Reconstr Surg. 2008. 122:340–347.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management based on grading of animation deformity following implant-based subpectoral breast reconstruction
- Prepectoral breast reconstruction
- Selection of Implants in Unilateral Prosthetic Breast Reconstruction and Contralateral Augmentation
- The Goldilocks technique: An alternative method to construct a breast mound after prosthetic breast reconstruction failure
- Mondor's Disease after Immediate Breast Reconstruction with Silicone Implant
