Nipple-areolar complex reconstruction: systematic approach
- Affiliations
-
- 1Department of Plastic & Reconstructive Surgery, Yonsei University College of Medicine, Seoul, Korea. dhlew@yuhs.ac
Abstract
- The goal of nipple-areolar reconstruction is to create a nipple that is appropriately located on the breast mound and has adequate projection, shape, color and texture to match the contralateral nipple-areolar complex. Despite various reports of techniques, no single technique is considered as an established method. The common methods of nipple reconstruction consist of composite grafts and local flaps, and the areolar is usually reconstructed by skin graft and tattooing. The authors introduce a systematic approach to select the appropriate reconstructive techniques for nipple-areolar complex reconstruction. If the patient has sufficient projection of the contralateral nipple and is willing to use it as a donor site, the composite graft of nipple is primarily considered. When the composite graft is not indicated, the methods using local flap such as skate flap and CV flap are proposed. Skate flap is best suited to maintain the contour of reconstructed breast mound. Although CV flap may distort the shape of breast mound, the method is popular for its simplicity. For creation of areolar, tattooing is widely performed to minimize the donor site morbidity rather than skin graft. Despite the algorithm of reconstructive techniques, it is important for the surgeon to choose the most familiar technique for superior outcomes. The nipple-areolar complex reconstruction is an integral step in the long treatment journey. Although the techniques of nipple reconstruction seem simplistic, they play a major role and demand meticulous attention to achieve good aesthetic outcomes.
Figure
-
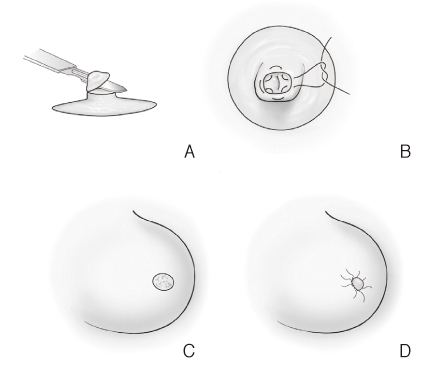
Figure 1 Nipple reconstruction by the composite graft. (A) Composite tissue is harvested from a contralateral nipple. (B) The donor site defect is primarily closed. (C) Deepithelialization is performed at the position of new nipple. (D) The composite tissue is grafted and tie-over dressing is performed to fix the grafted tissue firmly.
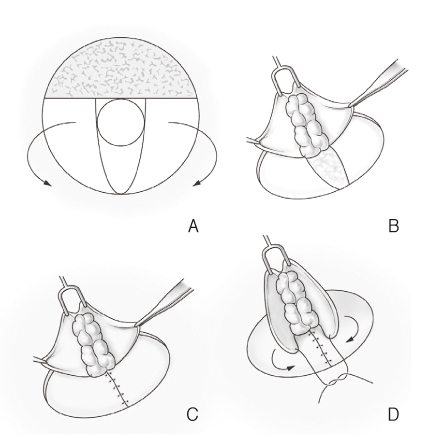
Figure 2 Nipple reconstruction by the skate flap. (A) The area beyond tangent to new nipple area is denuded. (B) Wings of skate are elevated with deep split thickness, and body is dissected centrally and elevated involving dermis and fat tissue. (C) The donor defect of body is primarily closed. (C) Deepithelialization is performed at the position of new nipple. (D) Wings of skate are brought around body each other to form nipple cone.
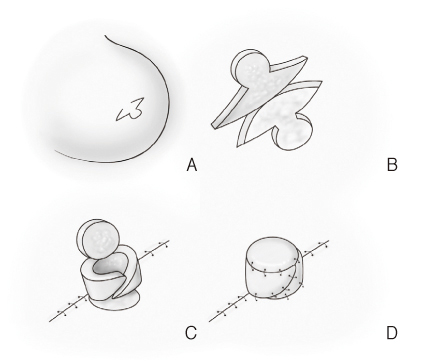
Figure 3 Nipple reconstruction by the CV flap. (A) The incision line of CV flap is drawn at the appropriate position of the reconstructed breast mound. (B) One C flap and two V flaps are elevated together preserving dermis and fat tissue. (C) The donor defects of V flaps are primarily closed, and two V flaps cross to form side wall. (D) The C flap covers the top of new nipple to complete to reconstruct a new nipple.
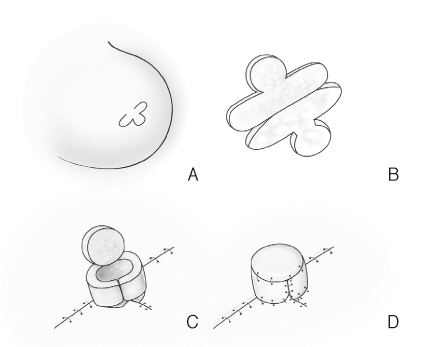
Figure 4 Nipple reconstruction by the CU flap. (A) The incision line of CU flap is drawn at the appropriate position of the reconstructed breast mound. The U flap has round tip and short flap length relative to V flap. (B) One C flap and two U flaps are elevated together preserving dermis and fat tissue. (C) The donor defects of C flap and V flaps are primarily closed, and a triangular flap is elevated as to insert between the U flaps. Tips of U flaps meet each other to form side wall. (D) The C flap cover the top of new nipple to complete to reconstruct a new nipple.
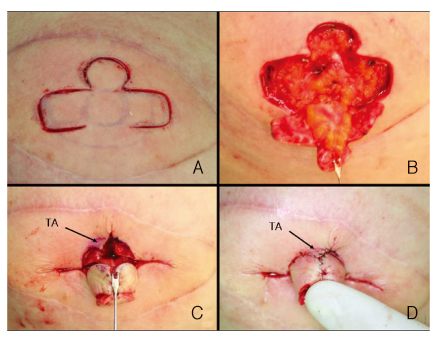
Figure 5 Nipple reconstruction by the CU flap. (A) The incision is made with CU shape. (B) The flaps are elevated and defattened except the base of flap. (C) The base of the nipple is deepithelized and a small triangular flap is elevated. (D) The triangular flap is transposed between the U flaps to prevent scar contracture. TA, triangular flap.
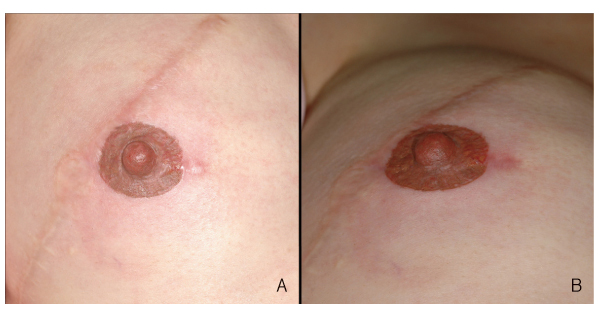
Figure 6 Nipple-areolar reconstruction. The nipple was reconstructed with CU flap method and the areolar tattooing was performed. (A) Frontal view. (B) Oblique view.

Figure 7 Completion of breast reconstruction with nipple-areolar reconstruction. (A) Preoperative view before nipple reconstruction. The breast mound was built with latissimus dorsi myocutaneous flap. (B,C,D) Postoperative view after nipple-areolar reconstruction. The nipple was reconstructed with CU flap method and the areolar tattooing was performed.
Reference
-
1. Yun IS, Lew DH, Tark KC. Nipple reconstruction with modified C-V flap: C-U flap. J Korean Soc Aesthetic Plast Surg. 2008. 14:75–78.2. Losken A, Mackay GJ, Bostwick J 3rd. Nipple reconstruction using the C-V flap technique: a long-term evaluation. Plast Reconstr Surg. 2001. 108:361–369.
Article3. Shestak KC, Gabriel A, Landecker A, Peters S, Shestak A, Kim J. Assessment of long-term nipple projection: a comparison of three techniques. Plast Reconstr Surg. 2002. 110:780–786.
Article4. Banducci DR, Le TK, Hughes KC. Long-term follow-up of a modified Anton-Hartrampf nipple reconstruction. Ann Plast Surg. 1999. 43:467–469.
Article5. Few JW, Marcus JR, Casas LA, Aitken ME, Redding J. Long-term predictable nipple projection following reconstruction. Plast Reconstr Surg. 1999. 104:1321–1324.6. Jabor MA, Shayani P, Collins DR Jr, Karas T, Cohen BE. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg. 2002. 110:457–463.
Article7. Kroll SS, Reece GP, Miller MJ, Evans GR, Robb GL, Baldwin BJ, Wang BG, Schusterman MA. Comparison of nipple projection with the modified double-opposing tab and star flaps. Plast Reconstr Surg. 1997. 99:1602–1605.
Article8. Guerra AB, Khoobehi K, Metzinger SE, Allen RJ. New technique for nipple areola reconstruction: arrow flap and rib cartilage graft for long-lasting nipple projection. Ann Plast Surg. 2003. 50:31–37.
Article9. Beckenstein MS. Thorne CH, Beasley RW, Aston SJ, Bartlett SP, Gurtner GC, Spear SL, editors. Nipple reconstruction. Grabb and Smith's plastic surgery. 2007. 6th ed. Philadelphia: Lippincott Williams & Wilkins;676–680.10. Nahabedian MY. Nipple reconstruction. Clin Plast Surg. 2007. 34:131–137.
Article11. Delay E, Mojallal A, Vasseur C, Delaporte T. Immediate nipple reconstruction during immediate autologous latissimus breast reconstruction. Plast Reconstr Surg. 2006. 118:1303–1312.
Article12. Mathes SJ, Ueno CM. Mathes SJ, Hentz VR, editors. Reconstruction of the nipple-areolar complex. Plastic surgery. 2006. 2nd ed. Philadelphia: Saunders Elsevier;791–818.13. Ahn ST. Ahn ST, editor. Algorithm for nipple-areolar reconstruction. Aesthetic and reconstructive breast surgery. 2010. Seoul: Koonja Publishing Co.;491–513.14. Spear SL, Arias J. Long-term experience with nipple-areola tattooing. Ann Plast Surg. 1995. 35:232–236.
Article15. Fourie le R, Bruce-Chwatt A. Professional tattooing: alternative method to nipple reconstruction. Br J Plast Surg. 2004. 57:693–694.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- VARIOUS METHODS OF NIPPLE AREOLAR RECONSTRUCTION
- Sequential breast and nipple-areolar complex reconstruction after soft tissue necrosis following augmentation mastopexy: a case report
- Skin - sparing Mastectomy with Circumareolar Incision and Immediate TRAM & One - stage Star Flap Nipple - areolar Complex Reconstruction
- Immediate Breast Reconstruction with TRAM Flap after Nipple-Areolar Sparing Mastectomy
- A Novel Nipple Reconstruction Technique for Maintaining Nipple Projection: The Boomerang Flap
