Endoscopic Decompression for Optic Neuropathy in McCune-Albright Syndrome
- Affiliations
-
- 1Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. shinhj@skku.edu
- KMID: 2339973
- DOI: http://doi.org/10.3340/jkns.2014.56.3.281
Abstract
- McCune-Albright syndrome (MAS) is characterized by a triad of poly/monostotic fibrous dysplasia, cafe-au-lait macules and hyperfunctioning endocrinopathies including human growth hormone excess. Acromegaly as a manifestation of endocrine hyperfunction with MAS is uncommon. Surgical excision may be challenging due to the associated severe fibrous dysplasia of the skull base. Through the endoscopic procedures, we treated a case of MAS presenting with compressive optic neuropathy due to fibrous dysplasia and acromegaly caused by growth hormone secreting pituitary adenoma. We reviewed the literature on GH excess in MAS to highlight its surgical and medical challenges.
MeSH Terms
Figure
-
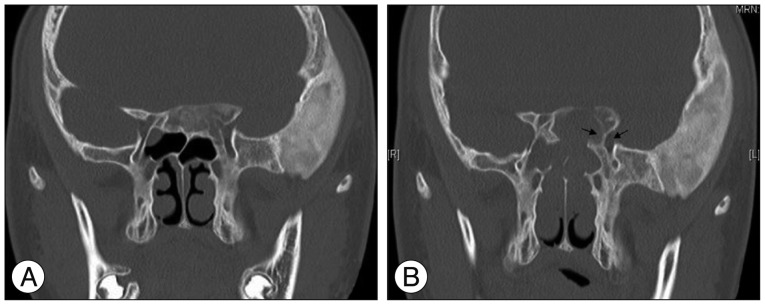
Fig. 1 Ostiometal unit (OMU) CT scan before and after optic nerve decompression. A : The non-contrast OMU CT scan demonstrates an expanded left basiocciput and greater sphenoid wing, typical for fibrous dysplasia. B : After endoscopic transnasal transsphenoidal and transethmoidal approach, postoperative OMU CT shows relief of left optic canal by removal of the fibrous lesion (arrows).
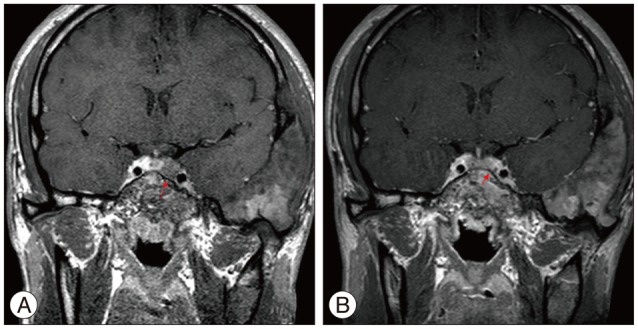
Fig. 2 Sellar magnetic resonance (MR) images performed before and after transsphenoidal tumor removal. A : Sellar magnetic resonance (MR) image performed before transsphenoidal tumor removal show slightly prominent posterior pituitary gland with newly developed mass-like lesion in the left side of pituitary gland which is measured about 7 mm, without definite enhancement (red arrow). B : The follow-up sellar MR image 1-year post-operatively demonstrates no residual tumor in the pituitary gland and no significant interval change in polyostotic fibrous dysplasia (red arrow).
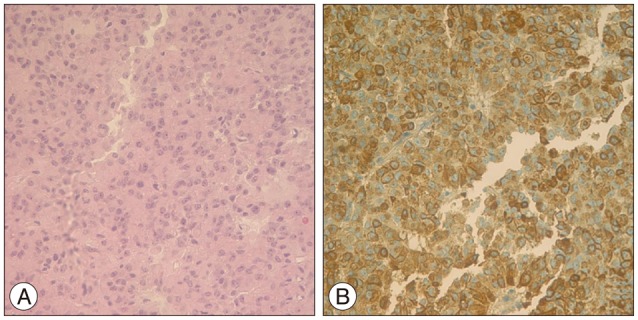
Fig. 3 Histopathology of pituitary adenoma. A : Histological examination revealed tumor cells with cytoplasmic, uniformly round, secretory granules of widely varying sizes on light microscopy, ×400. B : Immunohistochemistry for growth hormone (GH) with light hematoxylin counterstain, ×400. The majority of adenoma cells manifested GH immunoreactivity.
Reference
-
1. Akintoye SO, Chebli C, Booher S, Feuillan P, Kushner H, Leroith D, et al. Characterization of gsp-mediated growth hormone excess in the context of McCune-Albright syndrome. J Clin Endocrinol Metab. 2002; 87:5104–5112. PMID: 12414879.
Article2. Albright F, Butler AM, Hampton AO, Smith P. Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction, with precocious puberty in females : reports of five cases. N Engl J Med. 1937; 216:727–746.
Article3. Chanson P, Dib A, Visot A, Derome PJ. McCune-Albright syndrome and acromegaly : clinical studies and responses to treatment in five cases. Eur J Endocrinol. 1994; 131:229–234. PMID: 7921205.
Article4. Cremonini N, Graziano E, Chiarini V, Sforza A, Zampa GA. Atypical McCune-Albright syndrome associated with growth hormone-prolactin pituitary adenoma : natural history, long-term follow-up, and SMS 201-995--bromocriptine combined treatment results. J Clin Endocrinol Metab. 1992; 75:1166–1169. PMID: 1400888.
Article5. Dou W, Lin N, Ma W, Yang Y, Zhu H, Sun J, et al. Transsphenoidal surgery in a patient with acromegaly and McCune-Albright syndrome : application of neuronavigation. J Neurosurg. 2008; 108:164–169. PMID: 18173327.
Article6. Gessl A, Freissmuth M, Czech T, Matula C, Hainfellner JA, Buchfelder M, et al. Growth hormone-prolactin-thyrotropin-secreting pituitary adenoma in atypical McCune-Albright syndrome with functionally normal Gs alpha protein. J Clin Endocrinol Metab. 1994; 79:1128–1134. PMID: 7962285.
Article8. Madsen H, Borges MT, Kerr JM, Lillehei KO, Kleinschmidt-Demasters BK. McCune-Albright syndrome : surgical and therapeutic challenges in GH-secreting pituitary adenomas. J Neurooncol. 2011; 104:215–224. PMID: 21104108.
Article9. McCune DJ. Osteitis fibrosa cystica : the case of nine year old girl who also exhibits precocious puberty, multiple pigmentation of the skin and hyperthyroidism. Am J Dis Child. 1936; 52:743–747.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Orbital Decompression for Dysthyroid Optic Neuropathy
- Three Cases of Endoscopic Endonasal Optic Nerve Decompression for Nontraumatic Optic Neuropathy
- A Case of Ketoconazole Treatment in McCune-Albright Syndrome
- A case of McCune-Albright syndrome
- 2 Cases of Optic Nerve Decompression of Two Traumatic Optic Neuropathies Using Intranasal Endoscope
