Anticholinesterase Treatment for Patients With Paralytic Strabismus Following a Viper Bite
- Affiliations
-
- 1Department of Ophthalmology, Dongguk University Gyeongju Hospital, Gyeongju, Korea. letter0116@naver.com
Abstract
- PURPOSE
To describe the therapeutic effect of anticholinesterase treatment for patients with paralytic strabismus and blepharoptosis following a viper bite
METHODS
A prospective non-comparative interventional case series study was designed including 6 patients with ophthalmic complications such as paralytic strabismus and blepharoptosis following a viper bite. Anticholinesterase (pyridostigmine) 60 mg was administered to patients 3 times a day in additional to conservative treatment including antivenom, antibiotics and tetanus toxoid. Patients underwent a measurement of deviation, diplopia test and MRD 1. Subjective evaluation of the diplopia symptoms was performed daily after treatment.
RESULTS
Subjective diplopia was relieved in 2 out of the 6 patients on the first day and in the other 4 patients on the second day. The angle of deviation decreased approximately 37% on the first day and ocular position became orthophoric on the third day in all patients. The blepharoptosis was completely resolved in 4 patients on the first day. No complication following anticholinesterase treatment was noticed.
CONCLUSIONS
Treatment using anticholinesterase for patients suffering from diplopia and blepharoptosis following a viper bite is an effective and safe treatment.
MeSH Terms
Figure
-

Figure 1. Fang marks of patients on the left forearm (Case 2, A), the right middle finger (Case 3, B), the left ankle (Case 4, C) and the left thumb (Case 6, D) with an erythematous swelling and pain after a viper bite.

Figure 2. Nine cardinal photographs of 50-year-old male patient after a viper bite (Case 3, A) and 53-year-old male patient after a viper bite (Case 4, B). Exotropia at distance and the mild limitation of the left eye at right gaze.
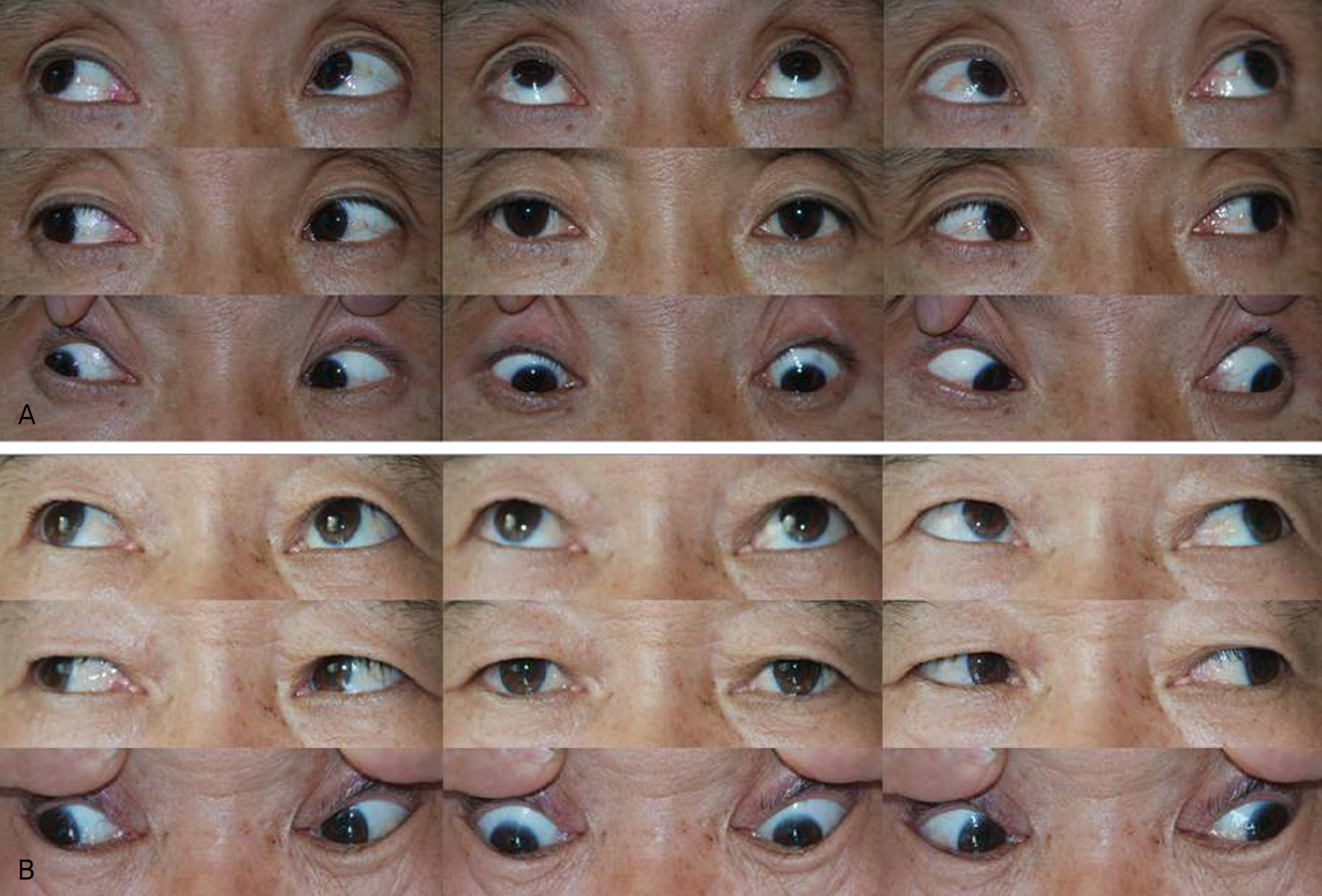
Figure 3. Nine cardinal photographs of same patients (Case 3, A), (Case 4, B). Exotropia and the limitation of the left eye were resolved after anticholinesterase treatment.

Figure 4. Photographs of a 50-year-old male patient after a viper bite (Case 3). The ptosis of both lid and paralytic exotropia at distance without the limitation of the eye movement (A) and the resolution of lid ptosis and paralytic exotropia after one day of anticholinesterase treatment (B).
Reference
-
References
1. Russell FE. Snake venom poisoning in the United States. Annu Rev Med. 1980; 31:247–59.
Article2. Ari AB. Patient with purely extraocular manifestation from a pit viper snakebite. Mil Med. 2001; 16:667–9.3. Moore TC. Snakebite from the Korean pit viper. Mil Med. 1977; 142:546–9.
Article4. Campbell CH. The effects of snake venoms and their neurotoxins on the nervous system of man and animals. Contemp Neurol Ser. 1975; 12:259–93.5. Yoon JW, Choi CD, Kwon MD, Choi YK. A case of visual distur-bance by viper bites. J Korean Ophthalmol Soc. 1970; 11:159–61.6. Sung CK, Ha MC. A case of extraocular muscle paresis by viper bite. J Korean Ophthalmol Soc. 1981; 22:261–3.7. Lee SW, Jung IC, Yoon YH, et al. Anticholinesterse therapy for patients with ophthalmoplegia following snake bites: report of two cases. J Korean Med Sci. 2004; 19:631–3.8. Paik NK, Son JR. The clinical character of Korean poisonous snake bite. J Korean Surg Soc. 1996; 51:119–27.9. Kinoshita T, Ohba N, Sasaki N. A case of bilateral medial rectus paresis following bite by a viper. Jpn J Clin Ophthalmol. 1998; 52:1741–3.10. Sugihara H, Nimura A, Kato T, Nikita T. Enzymochemical studies on snake venoms. X. Purification and properties of arginine ester hydrolase (ME-3) in the venom of Trimeresurus mucrosquamatus. Yakugaku Zasshi. 1982; 102:560–7.
Article11. Chang CC, Chen HM, Lin MF, Yang CC. Immunochemical studies on cobra venom toxin. Toxicon. 1976; 14:408–9.12. Cho IO, Chang SD, Lee SY. Paralytic exotropia from pit viper snakebite. J Korean Ophthalmol Soc. 2004; 45:1939–44.13. Von Noorden GK. Binocular vision and ocular motility. Theory and management of strabismus. 6th ed.St. Lous: C.V Mosby;2002. p. 101–13.14. Campolattaro BN, Wang FM. Anatomy and physiology of the extraocular muscles and surrounding tissues. 3th ed.Philadelpia: Mosby;1999. p. 6–8.15. Re G, Trisolino G, Miglio F. Eye muscle paralysis after Vipera aspis envenomation. J Accid Emerg Med. 1999; 16:458.
Article16. Antonini G, Rasura M, Conti G, Mattia C. Neuromuscular paralysis in Vipera aspis envenomation: pathogenetic mechanism. J Nerol Neurosurg Psychiatry. 1991; 54:187.17. Fauci AS, Braunwald E, Kasper DL, et al. Harrison's principles of internal medicine. 15th ed.New York: McGraw-Hill;2001. p. 382.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Paralytic Strabismus after a Snake Bite on the Toe
- Paralytic Exotropia from Pit Viper Snakebite
- Binocular Visual Rehabilitation in Paralytic Strabismus by Botulinum A Toxin Chemodenervation
- Botulinum Toxin A Chemodenervation in Strabismus
- The Effect of Botulinum Toxin Chemodenervation in Chronic Paralytic Strabismus
