J Korean Ophthalmol Soc.
2007 Dec;48(12):1742-1746.
A Case of Optic Neuritis in Acute Sphenoid Sinusitis
- Affiliations
-
- 1Department of Ophthalmology, Dongsan Hospital, College of Medicine, Keimyung University, Daegu, Korea. eyedr@dreamwiz.com
Abstract
-
PURPOSE: We encountered a rare case of optic neuritis that developed in a sphenoid sinusitis. This case has not been reported at any of the Korean Ophthalmological Society meetings.
CASE SUMMARY
A 12-year-old boy with swollen optic disc was diagnosed with optic neuritis secondary to sphenoid sinusitis, through orbit MRI (magnetic resonance imaging) and paranasal sinus CT (computed tomography). We observed the recovery of visual acuity and the improvement of papilledema after treatment. In the initial examination, the BCVA (best-corrected visual acuity) of the right eye was only hand movement. Papilledema was detected by ophthalmoscopy. Orbit MRI and paranasal sinus CT were then performed, which revealed that sphenoid sinusitis had invaded the right optic nerve. Treatment included the use of antibiotics, systemic steroid therapy, and endoscopic sinus surgery. One month after treatment, the BCVA of the right eye was 1.0 and the papilla of right eye had a normal ophthalmoscopic finding.
CONCLUSIONS
Sphenoid sinusitis can be a cause of optic neuritis. The treatment of optic neuritis caused by paranasal sinusitis must include antibiotics use or endoscopic sinus surgery to remove the sinus inflammation as well as high dose steroid therapy.
MeSH Terms
Figure
-

Figure 1. Optic disc on ophthalmoscopy. (A) Swollen optic disc due to optic neuritis before treatment, (B) Clear optic disc margin after endoscopic sinus surgery.

Figure 2. Preoperative paranasal sinus dynamic CT. The image shows low density of soft tissue lesion in the sphenoid sinus, and there is no bony erosion or destruction of the walls of the sphenoid sinus (axial view).
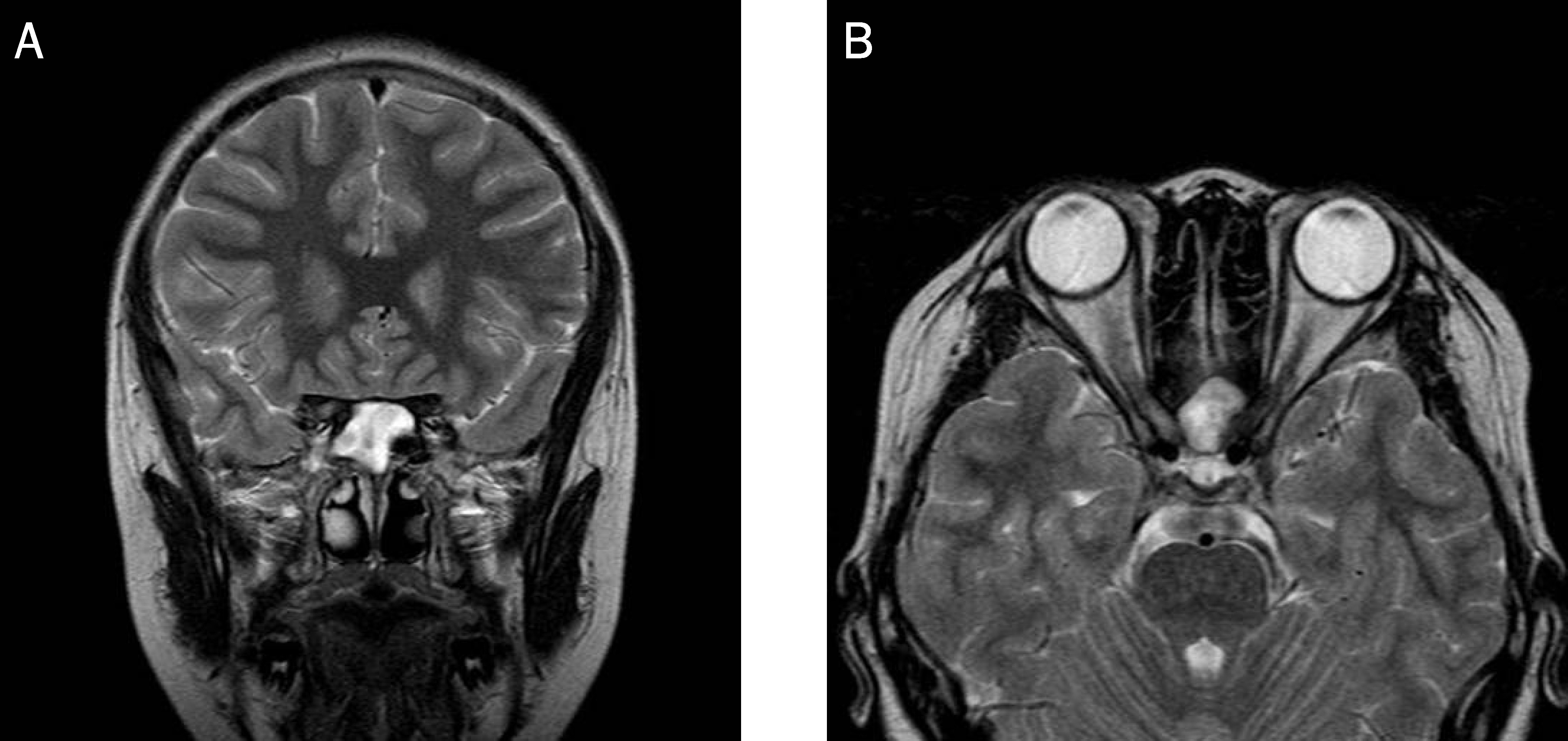
Figure 3. Preoperative orbit MRI scan (T2W1 image). (A) The sphenoid sinus is filled with high signal enhancement lesion (coronal view), (B) The image shows diffuse linear enhancement of the right optic nerve in the intraorbital and orbital apex region (axial view).
Reference
-
References
1. Jin YP, Pedro-Cuesta J, Soderstrom M, et al. Incidence of optic neuritis in Stockholm, Sweden 1990-1995, 1: age, sex, birth and ethnic-group related patterns. J Neurol Sci. 1998; 159:107–14.2. Kim TS, Kim JH, Nam YK. Bilateral optic neuritis following measles. J Korean Ophthalmol Soc. 2002; 43:1816–20.3. Ebers GC. Optic neuritis and multiple sclerosis. Arch Neurol. 1985; 42:702–4.
Article4. Optic Neuritis Study Group. The 5-year risk of MS after optic neuritis: Experience of the optic neuritis treatment trial. Neurology. 1997; 49:1404–13.5. Rothstein J, Maisel RH, Berlinger NT, et al. Relationship of optic neuritis to disease of the paranasal sinuses. Laryngoscope. 1984; 94:1501–8.
Article6. Hickmann SJ, Dalton CM, Miller DH, Plant GT. Management of acute optic neuritis. Lancet. 2002; 360:1953–62.7. Heron JR. Diagnosis of optic neuropathy. In : Hess RF, Plant GT, editors. Optic neuritis. 1st ed.New York: Cambridge University;1986. chap. 4.8. Morales DS, Siatkowski RM, Howard CW, et al. Optic Neuritis in Children. J Pediatr Ophthalmol Strabismus. 2000; 37:254–9.9. Hwang JM, Lee YJ, Kim MK. Optic Neuritis in Asian Children. J Pediatr Ophthalmol Strabismus. 2002; 39:26–39.
Article10. Lee YJ, Kim MK, Hwang JM. Optic neuritis in Children. J Korean Ophthalmol Soc. 2002; 43:314–9.11. Lew D, Southwick FS, Montgomery WW, et al. Sphenoid sinusitis. A review of 30 cases. N Engl J Med. 1983; 309:1149–54.12. Oh DE, Kim YD. Visual Loss due to Inflammatory Sinus Diseases. J Korean Ophthalmol Soc. 2006; 47:1879–86.13. Beck RW, Cleary PA. Optic neuritis treatment trial, One-year follow-up results. Arch Ophthalmol. 1993; 111:773–5.14. Beck RW. Walsh & Hoyt's Clinical Neuro-Ophthalmology. 5th ed.1. Baltimore: Williams & Wilkins;1998. p. 632–4.15. Chanzy S, Routon MC, Bursztyn J, et al. Maxillary and sphenoid sinusitis complicated by acute inflammatory neuritis in a 12-year-old patient. Arch Pediatr. 2005; 12:46–8.16. Back BJ, Kim HJ, Choi JH, Oh CH. A case of optic nerve decompression in a patient with retrobulbar neuritis secondary to paranasal sinusitis. Korean J Otolaryngol. 2000; 43:1355–8.17. Younis RT, Lazar RH, Bastillo A, Anand VK. Orbital infection as a complication of sinusitis: Are diagnosis and treatment trends changing? Management and treatment of complication of sinusitis in children. Ear Nose Throat J. 2002; 81:771–5.18. Lee LA, Huang CC, Lee TJ. Prolonged visual disturbance secondary to isolated sphenoid sinus disease. Laryngoscope. 2004; 114:986–90.
Article19. Kountakis SE, Maillard AA, Steinberg CM. Optic neuritis secondary to sphenoethmoiditis: Surgical treatment. Am J Otolaryngol. 1995; 16:422–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fungal Sphenoid Sinusitis with Visual Loss
- A Case of Optic Nerve Decompression in a Patient with Retrobulbar Neuritis Secondary to Paranasal Sinusitis
- A Case of Optic Neuritis Secondary to Fungal Sphenoid Sinusitis
- A Case of Fungal Sphenoidal Sinusitis Involving Optic Nerve
- A Case of Optic Neuropathy Caused by Sphenoid Sinus Mucocele
