J Korean Orthop Assoc.
2011 Oct;46(5):405-411.
Total Knee Replacement Arthroplasty with NexGen(R)-LPS: Minimum 5 Year Follow-up Results
- Affiliations
-
- 1Department of Orthopaedic Surgery, Inha University Hospital, Inha University School of Medicine, Incheon, Korea. moon@inha.ac.kr
Abstract
- PURPOSE
One hundred and thirty-six patients who underwent total knee replacement arthroplasty (TKRA) with NexGen(R)-LPS were analyzed for the clinical and radiologic results after a minimum follow-up of 5-years.
MATERIALS AND METHODS
This study included 136 patients (209 knees) who underwent TKRA with NexGen(R)-LPS between August 1998 and February 2005 and had a minimum follow-up of 5 years. We evaluated the range of motion (ROM), American Knee Society knee functional scores, radiographic results and complication rates in the study subjects with an average 8.3 years of follow-up (range: 5-11.5 years). We also compared the results of the degenerative arthritis group (195 knees in 129 patients) with those of the rheumatoid arthritis group (14 knees in 7 patients).
RESULTS
The mean ROM increased from 107.3degrees to 122degrees at the final follow-up. The flexion contracture also improved from 8.3degrees to 1.2degrees at final follow-up. The knee score improved from 51 to 94.7 at the final follow-up. The functional score improved from 38 to 84.2 (p<0.05) at final follow-up. There was no statistical significant difference in the results between the degenerative arthritis and rheumatoid arthritis groups (p>0.05). Valgus (alpha), varus (beta), flexion (gamma) and the posterior slope angle (delta) of the tibial components were well maintained both during the immediate postoperative period and at the final follow-up. There was no significant difference in the tibiofemoral angle and alpha, beta, gamma and delta angle (p>0.05) between the degenerative arthritis and rheumatoid arthritis groups. The alignment of the alternative substance was also relatively well maintained. Radiolucent lines were observed in 39 knees (18.7%), and in 42 zones out of 209 knees. The most common site of radiolucent lines was the medial side of the tibia in 21 knees. The overall incidence of radiolucent lines was 15% for the femur, 61% for the tibia and 24% for the patella. There was no statistically significant difference between the presence of radiolucent lines and the clinical results (p>0.05). There was 1 case of revision surgery due to loosening of implants at 8 years after surgery, but no early loosening was observed in the study subjects. Complications were found in 6 patients. Two patients with early postoperative infection were treated with revision surgery. Two patients with acute hematogenous infection 4 years after the initial operation were treated with revision surgery. Two patients with superficial infection were treated with antibiotics and regular dressing.
CONCLUSION
The patients treated with the NexGen(R)-LPS TKRA had a decreased level of postoperative pain and an improved knee joint ROM. A lower rate of complications was also found with this type of implant.
MeSH Terms
Figure
-
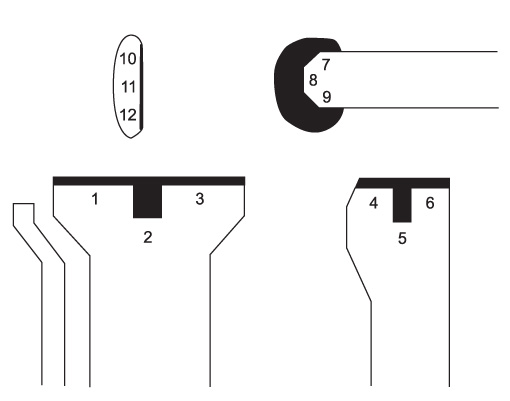
Figure 1 This diagram shows radiological evaluation and scoring system after TKRA.

Figure 2 Right anteroposterior knee radiograph shows radiolucent line (arrow).

Figure 3 (A) Right knee anteroposterior and lateral radiographs show a loose tibial implant with bone loss on the medial side of the tibia. (B) Radiographs after revision total knee arthroplasty.
Reference
-
1. Cross MJ, Parish EN. A hydroxyapatite-coated total knee replacement: prospective analysis of 1000 patients. J Bone Joint Surg Br. 2005. 87:1073–1076.2. Epinette JA, Manley MT. Hydroxyapatite-coated total knee replacement: clinical experience at 10 to 15 years. J Bone Joint Surg Br. 2007. 89:34–38.3. Oliver MC, Keast-Butler OD, Hinves BL, Shepperd JA. A hydroxyapatite-coated Insall-Burstein II total knee replacement: 11-year results. J Bone Joint Surg Br. 2005. 87:478–482.4. Banks S, Bellemans J, Nozaki H, Whiteside LA, Harman M, Hodge WA. Knee motions during maximum flexion in fixed and mobile-bearing arthroplasties. Clin Orthop Relat Res. 2003. 410:131–138.
Article5. Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T. Maximizing flexion after total knee arthroplasty: the need and the pitfalls. J Arthroplasty. 2002. 17:4 Suppl 1. 59–62.
Article6. Insall J, Scott WN, Ranawat CS. The total condylar knee prosthesis. A report of two hundred and twenty cases. J Bone Joint Surg Am. 1979. 61:173–180.
Article7. Knutson K, Lindstrand A, Lidgren L. Survival of knee arthroplasties. A nation-wide multicentre investigation of 8000 cases. J Bone Joint Surg Br. 1986. 68:795–803.
Article8. Kavolus CH, Ritter MA, Keating EM, Faris PM. Survivorship of cementless total knee arthroplasty without tibial plateau screw fixation. Clin Orthop Relat Res. 1991. 273:170–176.
Article9. Han CD, Shin SJ, Han DY. Radiologic analysis of cement-less total knee arthroplasty-comparative studies in osteoarthritis, rheumatoid arthritis. J Korean Knee Soc. 1996. 8:42–53.10. Hood RW, Wright TM, Burstein AH. Retrieval analysis of total knee prostheses: a method and its application to 48 total condylar prostheses. J Biomed Mater Res. 1983. 17:829–842.
Article11. Moon MS, Woo YK, Lee KH. Total knee replacement surgery for rheumatoid and osteoarthritic patients (comparative study). J Korean Orthop Assoc. 1991. 26:1165–1173.12. Ritter MA, Gioe TJ, Stringer EA, Littrell D. The posterior cruciate condylar total knee prosthesis. A five-year follow-up study. Clin Orthop Relat Res. 1984. 184:264–269.13. Scott RD, Volatile TB. Twelve years' experience with posterior cruciate-retaining total knee arthroplasty. Clin Orthop Relat Res. 1986. 205:100–107.
Article14. Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized condylar prosthesis: a modification of the total condylar design. Two to four-year clinical experience. J Bone Joint Surg Am. 1982. 64:1317–1323.15. Scott WN, Rubinstein M, Scuderi G. Results after knee replacement with a posterior cruciate-substituting prosthesis. J Bone Joint Surg Am. 1988. 70:1163–1173.
Article16. Dorr LD, Boiardo RA. Technical considerations in total knee arthroplasty. Clin Orthop Relat Res. 1986. 205:5–11.
Article17. Freeman MA, Railton GT. Should the posterior cruciate ligament be retained or resected in condylar nonmeniscal knee arthroplasty? The case for resection. J Arthroplasty. 1988. 3:Suppl. S3–S12.18. Kraay MJ, Meyers SA, Goldberg VM, Figgie HE 3rd, Conroy PA. "Hybrid" total knee arthroplasty with the Miller-Galante prosthesis. A prospective clinical and roentgenographic evaluation. Clin Orthop Relat Res. 1991. 273:32–41.19. Han HS, Kang SB, Yoon KS. High incidence of loosening of the femoral component in legacy posterior stabilised-flex total knee replacement. J Bone Joint Surg Br. 2007. 89:1457–1461.
Article20. Leone JM, Hanssen AD. Management of infection at the site of a total knee arthroplasty. J Bone Joint Surg Am. 2005. 87:2335–2348.
Article21. Rand JA, Ilstrup DM. Survivorship analysis of total knee arthroplasty. Cumulative rates of survival of 9200 total knee arthroplasties. J Bone Joint Surg Am. 1991. 73:397–409.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Knee Replacement Arthroplasty with Buechel and Pappas Knee: Minimum 2-Year Follow-up
- High-Flexion Total Knee Arthroplasty Using NexGen LPS-Flex System: Minimum 5-year Follow-up Results
- Results of Total Knee Arthroplasty with NexGen LPS-flex Implant Using Navigation System (Brain Lab): Results with a 5-year Follow-up
- A Comparison of the Short-term Results between the PCL Sacrificing Medial Pivot Knee and Nexgen(R) LPS Total Knee Arthroplasty
- Total Knee Arthroplasty with NexGen(R) System: Minimum Two Years Follow up Results
