J Dent Anesth Pain Med.
2016 Jun;16(2):103-109. 10.17245/jdapm.2016.16.2.103.
Identifying the more suitable nostril for nasotracheal intubation using radiographs
- Affiliations
-
- 1Department of Dental Anesthesiology, School of Dentistry, Seoul National University, Seoul, Korea. stone90@snu.ac.kr
- 2Department of Pediatric Dentistry, Seoul National University School of Dentistry, Seoul, Korea.
- KMID: 2328852
- DOI: http://doi.org/10.17245/jdapm.2016.16.2.103
Abstract
- BACKGROUND
One nostril must be selected for nasotracheal intubation. In some cases, structural anomalies within the nasal cavity hinder the insertion of the tube or complications, such as epistaxis, develop. This study examined the possibility of using radiography to select the nostril that would induce fewer complications.
METHODS
Four hundred and five patients who underwent nasotracheal intubation under general anesthesia were studied. A 7.0-mm internal diameter nasal right angle endotracheal (RAE) tube and 6.5-mm internal diameter nasal RAE tube were inserted into men and women, respectively. Complications were considered to have developed in cases in which insertion of the tube into the nasal cavity failed or epistaxis occurred. The tube was inserted into the other nostril for insertion failures and hemostasis was performed in cases of epistaxis. The degree of nasal septal deviation was determined from posteroanterior skull radiographs or panoramic radiographs; the incidence of complications was compared depending on the direction of the septal deviation and the intubated nostril.
RESULTS
The radiographs of 390 patients were readable; 94 had nasal septum deviation. The incidence of complications for cases without nasal septum deviation was 16.9%, that for cases in which the tube was inserted into the nostril on the opposite side of the deviation was 18.5%, and that for cases in which the tube was inserted into the nostril with the deviation was 35.0%, showing a high incidence of complications when intubation is performed through the nostril with septum deviation (chi-square test, P < 0.05 ).
CONCLUSIONS
Although there were no differences in the incidence rates of complications between intubation through the left nostril and that through the right nostril, radiological findings indicated that incidence of complications significantly increased when the tube was inserted into the nostril with the septum deviation.
MeSH Terms
Figure
-

Fig. 1 Panoramic radiographs.
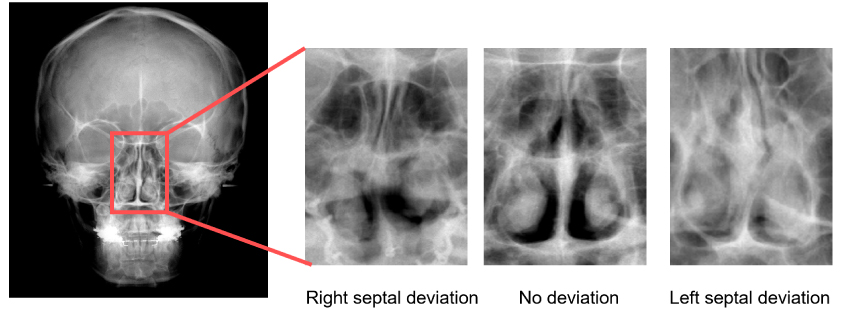
Fig. 2 Posteroanterior skull radiographs.
Reference
-
1. Dost P, Armbruster W. Nasal turbinate dislocation caused by nasotracheal intubation. Acta Anaesthesiol Scand. 1997; 41:795–796.2. Wilkinson JA, Mathis RD, Dire DJ. Turbinate destruction--a rare complication of nasotracheal intubation. J Emerg Med. 1986; 4:209–212.3. Binning R. Letter: A hazard of blind nasal intubation. Anaesthesia. 1974; 29:366–367.4. Smith JE, Reid AP. Identifying the more patent nostril before nasotracheal intubation. Anaesthesia. 2001; 56:258–262.5. Coe TR, Human M. The peri-operative complications of nasal intubation: A comparison of nostril side. Anaesthesia. 2001; 56:447–450.
Article6. Holdgaard HO, Pedersen J, Schurizek BA, Melsen NC, Juhl B. Complications and late sequelae following nasotracheal intubation. Acta Anaesthesiol Scand. 1993; 37:475–480.
Article7. Enk D, Palmes AM, Van Aken H, Westphal M. Nasotracheal intubation: A simple and effective technique to reduce nasopharyngeal trauma and tube contamination. Anesth Analg. 2002; 95:1432–1436. table of contents.
Article8. Read DH, Du Boulay M. A nasotracheal tube for faciomaxillary surgery. Anaesthesia. 1982; 37:940–943.
Article9. Lu PP, Liu HP, Shyr MH, Ho AC, Wang YL, Tan PP, et al. Softened endothracheal tube reduces the incidence and severity of epistaxis following nasotracheal intubation. Acta Anaesthesiol Sin. 1998; 36:193–197.
Article10. O'Hanlon J, Harper KW. Epistaxis and nasotracheal intubation--prevention with vasoconstrictor spray. Ir J Med Sci. 1994; 163:58–60.
Article11. Elwood T, Stillions DM, Woo DW, Bradford HM, Ramamoorthy C. Nasotracheal intubation: A randomized trial of two methods. Anesthesiology. 2002; 96:51–53.
Article12. Seo KS, Kim JH, Yang SM, Kim HJ, Bahk JH, Yum KW. A new technique to reduce epistaxis and enhance navigability during nasotracheal intubation. Anesth Analg. 2007; 105:1420–1424.
Article13. Lim CW, Min SW, Kim CS, Chang JE, Park JE, Hwang JY. The use of a nasogastric tube to facilitate nasotracheal intubation: A randomised controlled trial. Anaesthesia. 2014; 69:591–597.
Article14. Sanuki T, Hirokane M, Kotani J. Epistaxis during nasotracheal intubation: A comparison of nostril sides. J Oral Maxillofac Surg. 2010; 68:618–621.
Article15. Seo KS, Joo LA, Ko SJ, Kim HJ, Yum KW. The clinical study for epistaxis and tube insertion failure incidence on the choice of nostril during nasotracheal intubation. J Korean Dent Soc Anesthesiol. 2005; 5:107–111.
Article16. Lim HS, Kim D, Lee J, Son JS, Lee JR, Ko S. Reliability of assessment of nasal flow rate for nostril selection during nasotracheal intubation. J Clin Anesth. 2012; 24:270–274.
Article17. Harvey DC, Amorosa P. Traumatic nasotracheal intubation. Anaesthesia. 1986; 41:442.
Article18. Mahmood S, Lowe T. Management of epistaxis in the oral and maxillofacial surgery setting: An update on current practice. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:23–29.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Study for Epistaxis and Tube Insertion Failure Incidence on the Choice of Nostril during Nasotracheal Intubation
- Difference between Cardiovascular Response Blockades by Orolaryngeal and Nasal Lidocaine Sprays during Nasotracheal Intubation under Direct Laryngoscopy
- Retropharyngeal Dissection during Nasotracheal Intubation: A Case Report
- The Effect of Laryngeal View Grade and Intraoral Bleeding on Intubation Difficulty during Fiberoptic Nasotracheal Intubation
- Clinical Applications of the Balloon Dilation Technique during the Insertion of the Nasotracheal Tube
