Relation of Bony Carotid Canal Diameter and Clinical Manifestations in Patients with Moyamoya Disease
- Affiliations
-
- 1Department of Neurology, Kangdong Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea.
- 2Department of Neurology, Chuncheon Sacred Heart Hospital, College of Medicine, Chuncheon, Korea. dohchi@hallym.or.kr
- KMID: 2328820
- DOI: http://doi.org/10.14253/kjcn.2016.18.1.1
Abstract
- BACKGROUND
Moyamoya disease is characterized by a progressive stenosis or occlusion of the intracranial internal carotid artery and/or the proximal portion of the anterior cerebral artery and middle cerebral artery. Whether the onset time was childhood or adulthood, the bony carotid canal diameter might be different, but reflects the size of internal carotid artery passing through the bony carotid canal. In this study, we aimed to identify the relationship between bony carotid canal diameter and clinical manifestation.
METHODS
146 consecutive patients diagnosed with moyamoya disease by brain imaging studies were included. We measured the diameter of a transverse portion of bony carotid canal on bone window of a brain computed tomography(CT) image. Patients were divided into two groups, ischemic or hemorrhagic stroke according to clinical manifestation. As a result, 115 patients were included. The Suzuki stage was used as criteria for disease progression.
RESULTS
Bony carotid canal diameter was 3.6 ± 0.5 (right) and 3.6 ± 0.4 (left) in the hemorrhagic stroke group, and 3.7 ± 0.4 (right) and 3.6 ± 0.4 (left) in the ischemic stroke group. The bony carotid canal diameter of the moyamoya vessels (3.6 mm) was smaller than the diameter of non-moyamoya vessels (3.8 mm), significantly (p= 0.042). However, there was no difference in the collateral patterns and clinical manifestation in a comparison of both groups.
CONCLUSIONS
In our study, there was no significant difference of clinical manifestations and collateral patterns depend on the bony carotid canal diameter in patients with moyamoya disease. These findings suggest that the clinical presentations of moyamoya disease are not related to the onset time of the disease.
Keyword
MeSH Terms
Figure
-
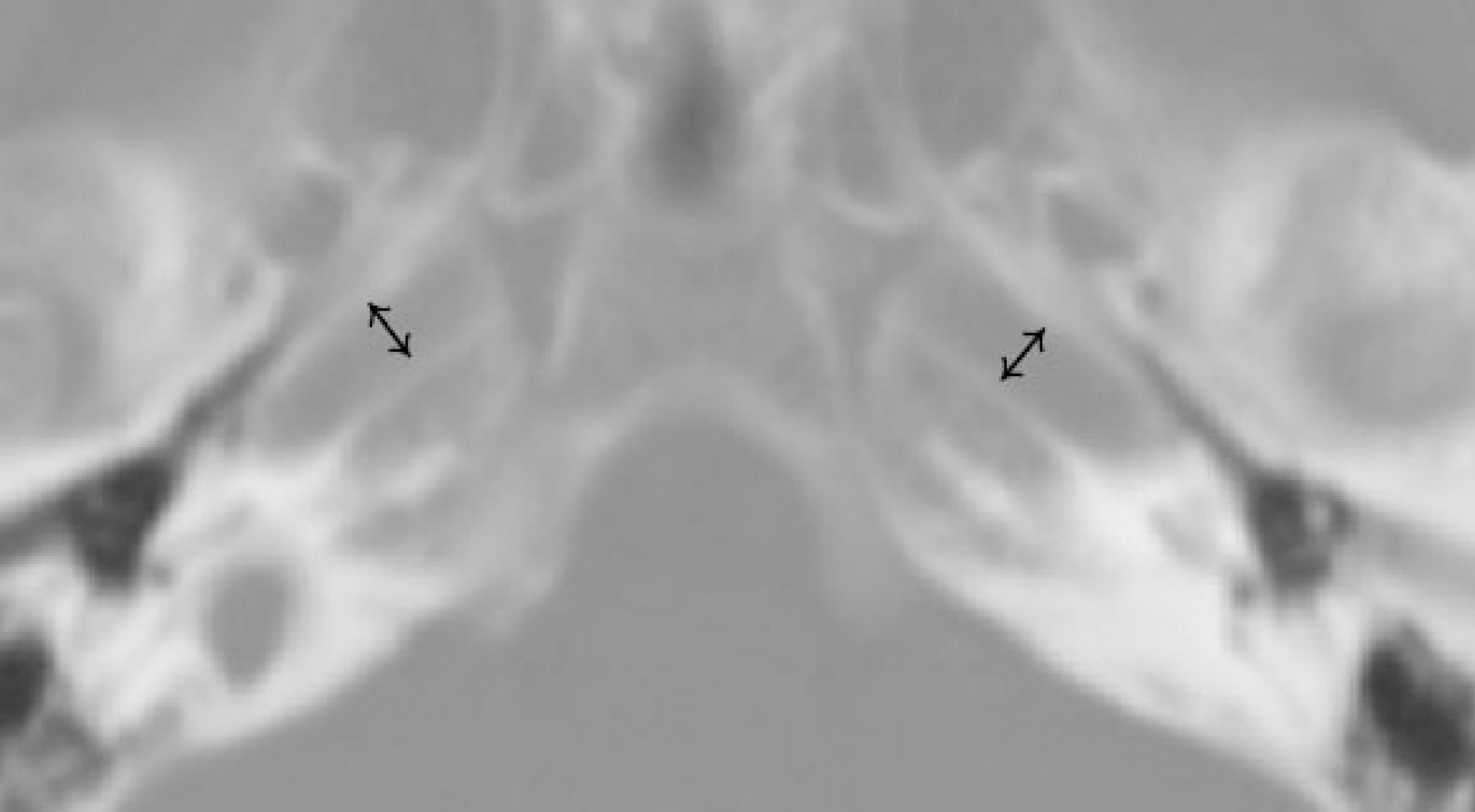
Figure 1. Measurement of bony carotid canal diameter. Bony carotid canal diameter was measured by transverse portion of bony carotid canal on bone window setting of brain CT (diameter of bidirectional arrow). CT; computed tomography.
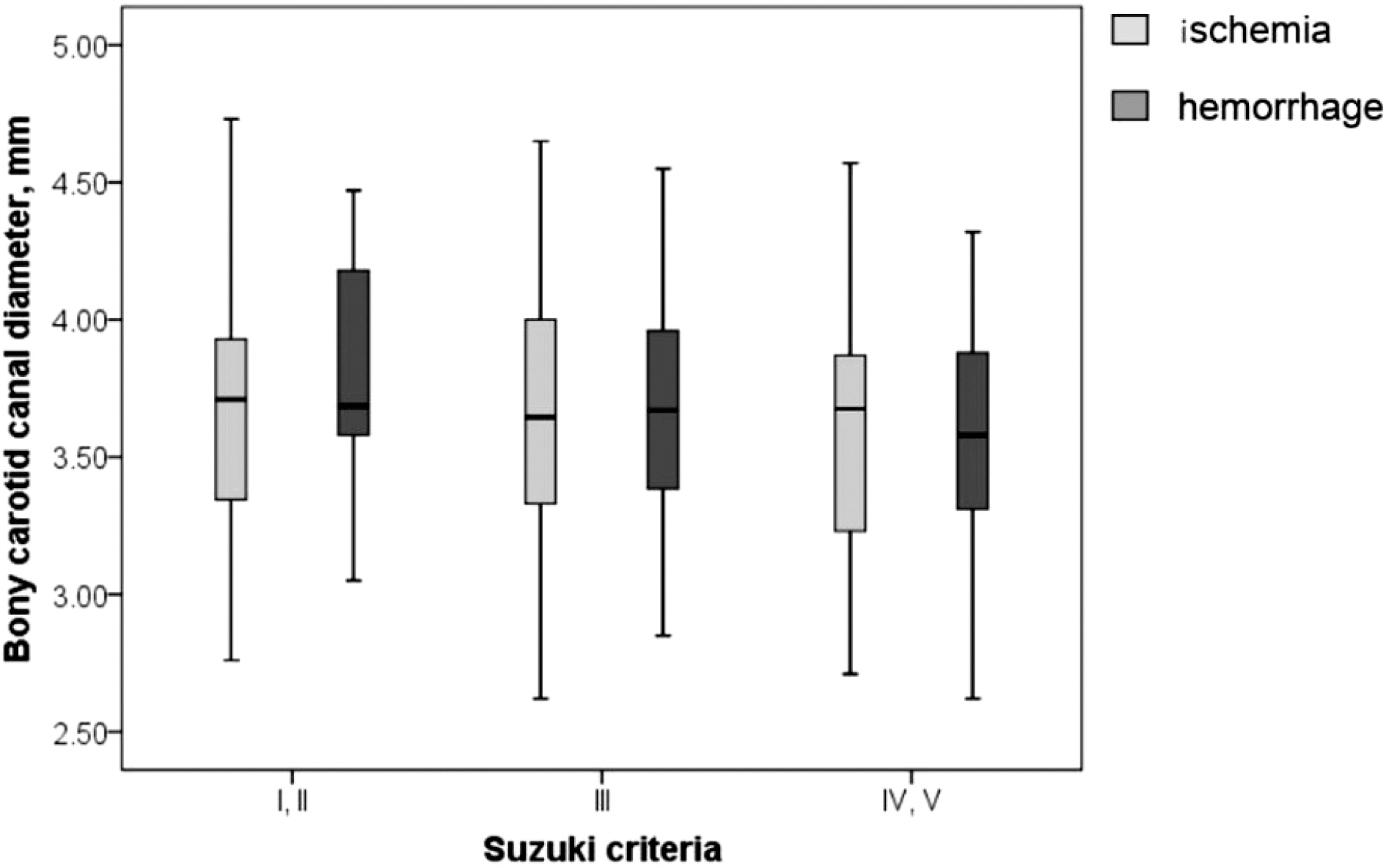
Figure 2. Relations of Suzuki stages and bony carotid canal diameter. Bony carotid canal diameter was compared in each ischemic and hemorrhage group according to Suzuki criteria.

Figure 3. Relations of bony carotid canal size and collateral patterns. Bony carotid canal size was divided into two groups. Average of moyamoya disease vessel diameter (3.6 mm) was the standard of small and large groups. Each group showed different collateral patterns. BCC; bony carotid canal.
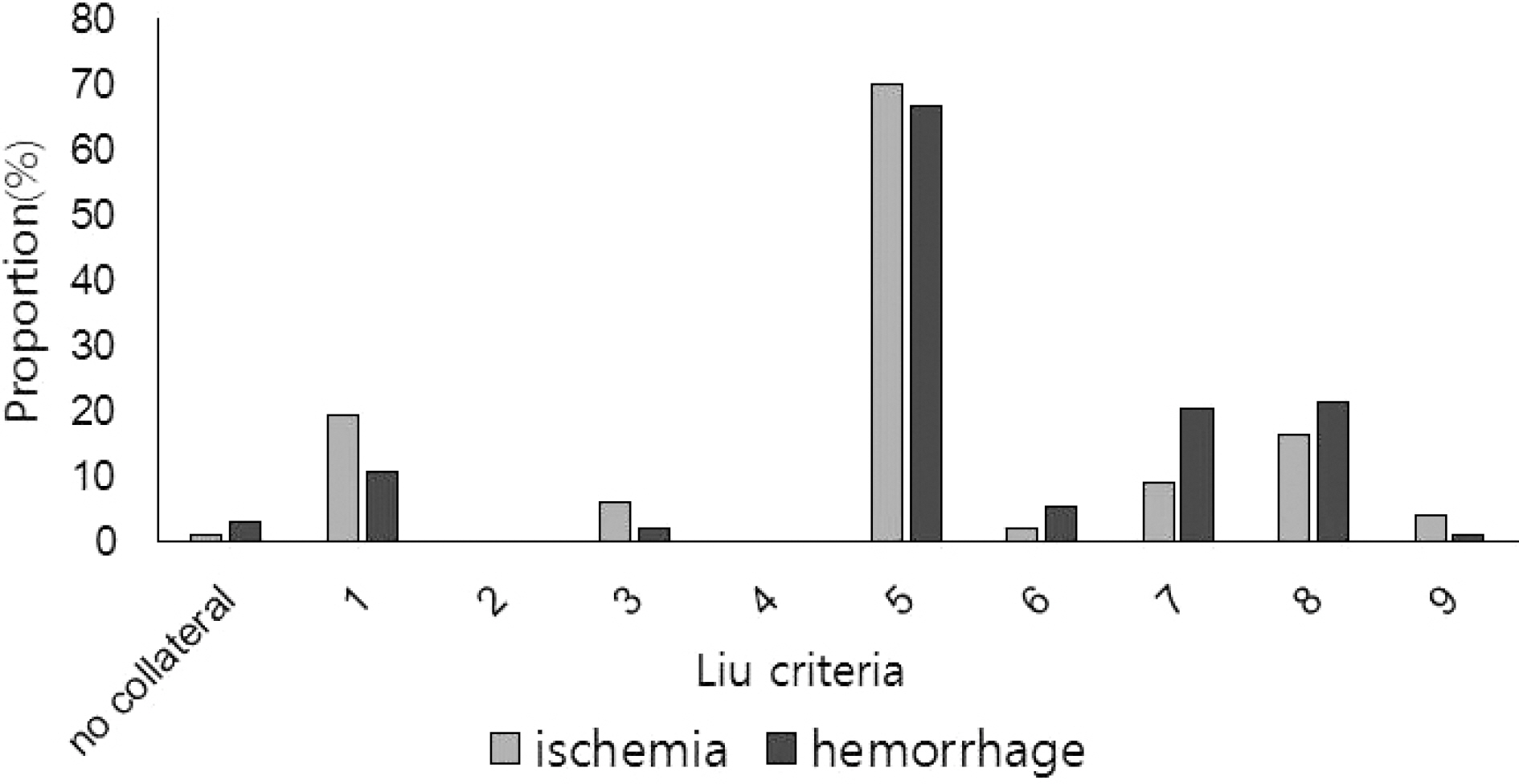
Figure 4. Relations of clinical manifestation and collateral patterns. Clinical manifestation was divided into two groups, ischemic and hemorrhagic stroke group. Each group showed different collateral patterns.
Reference
-
1.Guey S., Tournier-Lasserve E., Herve D., Kossorotoff M. Moyamoya disease and syndromes: from genetics to clinical management. Appl Clin Genet. 2015. 8:49–68.2.Hertza J., Loughan A., Perna R., Davis AS., Segraves K., Tiberi NL. Moyamoya disease: a review of the literature. Appl Neuropsychol Adult. 2014. 21:21–27.
Article3.Baba T., Houkin K., Kuroda S. Novel epidemiological features of moyamoya disease. J Neurol Neurosurg Psychiatry. 2008. 79:900–904.
Article4.Han DH., Kwon OK., Byun BJ., Choi BY., Choi CW., Choi JU, et al. A co-operative study: clinical characteristics of 334 Korean patients with moyamoya disease treated at neurosurgical institutes (1976-1994). The Korean Society for Cerebrovascular Disease. Acta Neurochir (Wien). 2000. 142:1263–1273.5.Wakai K., Tamakoshi A., Ikezaki K., Fukui M., Kawamura T., Aoki R, et al. Epidemiological features of moyamoya disease in Japan: findings from a nationwide survey. Clin Neurol Neurosurg. 1997. 99(Suppl 2):S1-S5.
Article6.Motoshima S., Noguchi T., Kawashima M., Ooishi M., Irie H., Nishihara M, et al. Narrowed petrous carotid canal detection for the early diagnosis of moyamoya disease. Fukuoka Igaku Zasshi. 2012. 103:206–214.7.Watanabe A., Omata T., Koizumi H., Nakano S., Takeuchi N., Kinouchi H. Bony carotid canal hypoplasia in patients with moyamoya disease. J Neurosurg Pediatr. 2010. 5:591–594.
Article8.Fukui M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (‘moyamoya' disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin Neurol Neurosurg. 1997. 99(Suppl 2):S238-S240.9.Hashimoto N., Tominaga T., Miyamoto S., Nagata I., Houkin K., Suzuki N, et al. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo). 2012. 52:245–266.10.Suzuki J., Takaku A. Cerebrovascular “moyamoya” disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol. 1969. 20:288–299.11.Liu W., Xu G., Liu X. Neuroimaging diagnosis and the collateral circulation in moyamoya disease. Interv Neurol. 2013. 1:77–86.
Article12.Cali RL., Berg R., Rama K. Bilateral internal carotid artery agenesis: a case study and review of the literature. Surgery. 1993. 113:227–233.13.Handa J., Matsuda I., Nakasu S., Nakano Y. Agenesis of an internal carotid artery: angiographic, tomographic and computed tomographic correlation. Neuroradiology. 1980. 19:207–211.
Article14.Quint DJ., Silbergleit R., Young WC. Absence of the carotid canals at skull base CT. Radiology. 1992. 182:477–481.
Article15.Fujimura M., Mugikura S., Shimizu H., Tominaga T. Asymptomatic moyamoya disease subsequently manifesting as transient ischemic attack, intracerebral hemorrhage, and subarachnoid hemorrhage in a short period: case report. Neurol Med Chir (Tokyo). 2010. 50:316–319.16.He Y., Zhou Q., He M. An asymptomatic Moyamoya disease: autopsy case and literature review. Am J Forensic Med Pathol. 2010. 31:77–79.17.Ikeda K., Iwasaki Y., Kashihara H., Hosozawa K., Anan K., Tamura M, et al. Adult moyamoya disease in the asymptomatic Japanese population. J Clin Neurosci. 2006. 13:334–338.
Article18.Jo KI., Yeon JY., Hong SC., Kim JS. Clinical course of asymptomatic adult moyamoya disease. Cerebrovasc Dis. 2014. 37:94–101.
Article19.Kuroda S., Ishikawa T., Houkin K., Nanba R., Hokari M., Iwasaki Y. Incidence and clinical features of disease progression in adult moyamoya disease. Stroke. 2005. 36:2148–2153.
Article
