The Influence of Metastatic Lymph Node Ratio on the Treatment Outcomes in the Adjuvant Chemoradiotherapy in Stomach Tumors (ARTIST) Trial: A Phase III Trial
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hematoma@skku.edu
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2328077
- DOI: http://doi.org/10.5230/jgc.2016.16.2.105
Abstract
- PURPOSE
In the Adjuvant Chemoradiotherapy in Stomach Tumors (ARTIST) trial, we investigated whether chemoradiotherapy after D2 gastrectomy reduces the rate of recurrence. Recently, the ratio of metastatic lymph nodes to examined lymph nodes (N ratio) has been proposed as an independent prognostic factor in gastric cancer (GC). The aim of this study was to investigate the relationship between the metastatic N ratio and prognosis of GC after curative D2 surgery.
MATERIALS AND METHODS
We retrospectively reviewed the data of 458 ARTIST patients who underwent D2 gastrectomy followed by adjuvant chemotherapy (XP, n=228) or chemoradiotherapy (XPRT, n=230). The disease-free survival (DFS) rates of patients were used to evaluate the influence of N ratio on the treatment outcome. To achieve this, 4 different N ratio categories (0%, 1%~9%, 10%~25%, and >25%) were compared on the basis of their influence on the treatment outcome.
RESULTS
On multivariate analysis, the N ratio remained an independent prognostic factor for DFS. The hazard ratios (HRs) for the N ratio categories of 0%, 1%~9%, 10%~25%, and >25% were 1, 1.061, 1.202, and 3.571, respectively. In patients having N ratio >25%, the 5-year DFS rates were 55% and 28% for the XPRT and XP arms, respectively (HR, 0.527; 95% confidence interval, 0.307~0.904; P=0.020).
CONCLUSIONS
In patients with curatively resected GC, the N ratio was independently associated with DFS. Although this finding warrants further investigation in future prospective studies, the benefit of chemoradiotherapy for D2 resected GC appears to be more beneficial in cancers having N ratios >25%.
Keyword
MeSH Terms
Figure
-
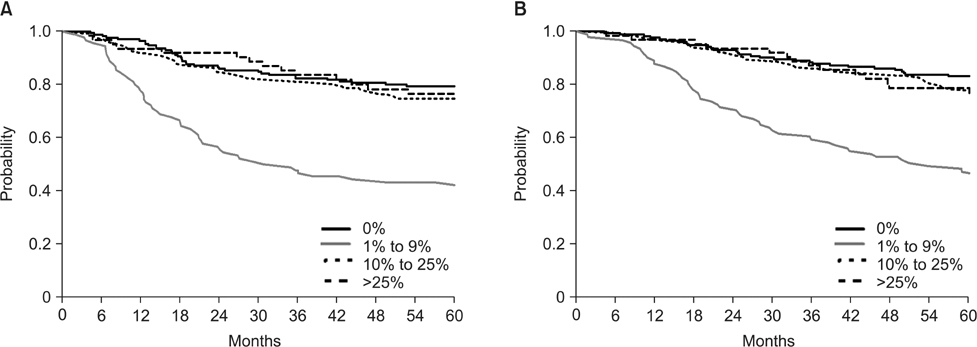
Fig. 1 (A) Disease-free survival curves according to N ratio. (B) Overall survival curves according to N ratio. The cut-off values for the N ratios are as follows: solid (black) line, 0%; dashed line, 1~9%; dotted line, 10~25%; and solid (gray) line, >25%. N ratio = the ratio of metastatic lymph nodes to examined lymph nodes.

Fig. 2 (A) Disease-free survival curves for patients with N ratios of 0%~25%. (B) Overall survival curves for patients with N ratios of 0%~25%. Solid line, XPRT arm; dotted line, XP arm. XP = capecitabine plus cisplatin; XPRT = concurrent chemoradiotherapy with XP; N ratio = the ratio of metastatic lymph nodes to examined lymph nodes.
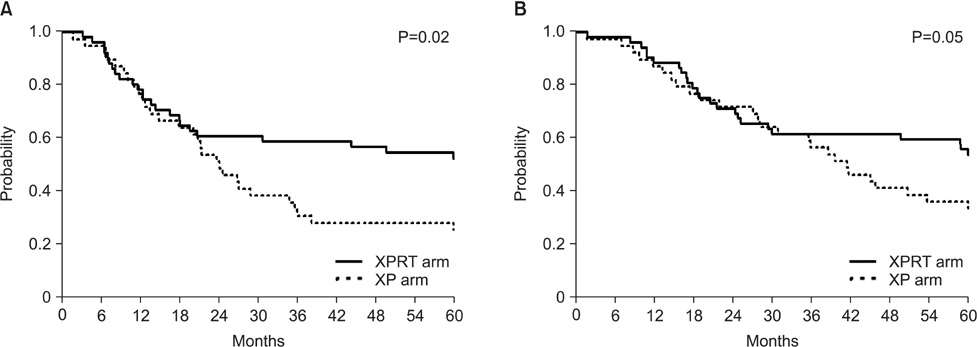
Fig. 3 (A) Disease-free survival curves for patients with N ratios >25% (B) Overall survival curves for patients with N ratios >25%. Solid line, XPRT arm; dotted line, XP arm. XP = capecitabine plus cisplatin; XPRT = concurrent chemoradiotherapy with XP; N ratio = the ratio of metastatic lymph nodes to examined lymph nodes.
Reference
-
1. Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010; 11:439–449.2. Sasako M, Sakuramoto S, Katai H, Kinoshita T, Furukawa H, Yamaguchi T, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011; 29:4387–4393.3. Noh SH, Park SR, Yang HK, Chung HC, Chung IJ, Kim SW, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014; 15:1389–1396.4. Lee J, Lim do H, Kim S, Park SH, Park JO, Park YS, et al. Phase III trial comparing capecitabine plus cisplatin versus capecitabine plus cisplatin with concurrent capecitabine radiotherapy in completely resected gastric cancer with D2 lymph node dissection: the ARTIST trial. J Clin Oncol. 2012; 30:268–273.5. Park SH, Sohn TS, Lee J, Lim DH, Hong ME, Kim KM, et al. Phase III trial to compare adjuvant chemotherapy with capecitabine and cisplatin versus concurrent chemoradiotherapy in gastric cancer: final report of the adjuvant chemoradiotherapy in stomach tumors trial, including survival and subset analyses. J Clin Oncol. 2015; 33:3130–3136.6. Ajani JA, Bentrem DJ, Besh S, D'Amico TA, Das P, Denlinger C, et al. Gastric cancer, version 2.2013: featured updates to the NCCN Guidelines. J Natl Compr Canc Netw. 2013; 11:531–546.7. Marchet A, Mocellin S, Ambrosi A, de Manzoni G, Di Leo A, Marrelli D, et al. The prognostic value of N-ratio in patients with gastric cancer: validation in a large, multicenter series. Eur J Surg Oncol. 2008; 34:159–165.8. Costa Junior WL, Coimbra FJ, Batista TP, Ribeiro HS, Diniz AL. Evaluation of N-ratio in selecting patients for adjuvant chemoradiotherapy after D2-gastrectomy. Arq Gastroenterol. 2013; 50:257–263.9. Nitti D, Marchet A, Olivieri M, Ambrosi A, Mencarelli R, Belluco C, et al. Ratio between metastatic and examined lymph nodes is an independent prognostic factor after D2 resection for gastric cancer: analysis of a large European monoinstitutional experience. Ann Surg Oncol. 2003; 10:1077–1085.10. Coimbra FJ, Costa WL Jr, Montagnini AL, Diniz AL, Ribeiro HS, Silva MJ, et al. The interaction between N-category and N-ratio as a new tool to improve lymph node metastasis staging in gastric cancer: results of a single cancer center in Brazil. Eur J Surg Oncol. 2011; 37:47–54.11. Kunisaki C, Shimada H, Nomura M, Matsuda G, Otsuka Y, Ono H, et al. Clinical impact of metastatic lymph node ratio in advanced gastric cancer. Anticancer Res. 2005; 25:1369–1375.12. Lee CM, Park SS, Kim JH. Current status and scope of lymph node micrometastasis in gastric cancer. J Gastric Cancer. 2015; 15:1–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Adjuvant Radiotherapy for Patients with Gastric Adenocarcinoma
- Results from the safety interim analysis of the adjuvant chemoradiotherapy in stomach tumors 2 trial: a multicenter, randomized phase III clinical trial
- Adjuvant Chemotherapy with or without Concurrent Radiotherapy for Patients with Stage IB Gastric Cancer: a Subgroup Analysis of the Adjuvant Chemoradiotherapy in Stomach Tumors (ARTIST) Phase III Trial
- Preoperative Chemotherapy in Advanced Stomach Cancer (Pros)
- Adjuvant Chemotherapy in Gastric Cancer
