Successful Treatment of Newly Developed, Intractable Digital Ulcers and Gangrene with Bosentan in Systemic Sclerosis
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea. gtah@hanmail.net
- 2Department of Nuclear Medicine, Kosin University College of Medicine, Busan, Korea.
- 3Department of Rheumatology, Pusan National University Hospital, Busan, Korea.
- KMID: 2326736
- DOI: http://doi.org/10.4078/jrd.2016.23.3.193
Abstract
- In systemic sclerosis, digital ulcers and gangrene are somewhat common clinical characteristics of obliterative vasculopathy. These manifestations increase morbidities, such as pain, infections, and acroosteolysis. However, patient responses to the appropriate treatments are often inadequate. We treated a patient with systemic sclerosis who had a refractory digital ulcer and gangrene with bosentan, an endothelin receptor antagonist, and observed improvement. Here we systematically review this case.
Keyword
MeSH Terms
Figure
-

Figure 1. Clinical course of digital ulcer. (A) An ulcer with pain had developed on the tip of her right middle finger by her first visit.(B) Six weeks after the first visit, despite using beraprost, the ulcer had worsened. Her treatment was switched to intravenous alprostadil. (C) Ten weeks after the first visit, the fingertip ulcer had deteriorated to gangrene (red arrow), despite the use of alprostadil for four weeks. Moreover, a new ulcer on the lateral side of the finger was noted (arrowhead). At this time, alprostadil was switched to bosentan. (D) Her digital ulcers and gangrene had improved after 10 weeks of bosentan treatment.
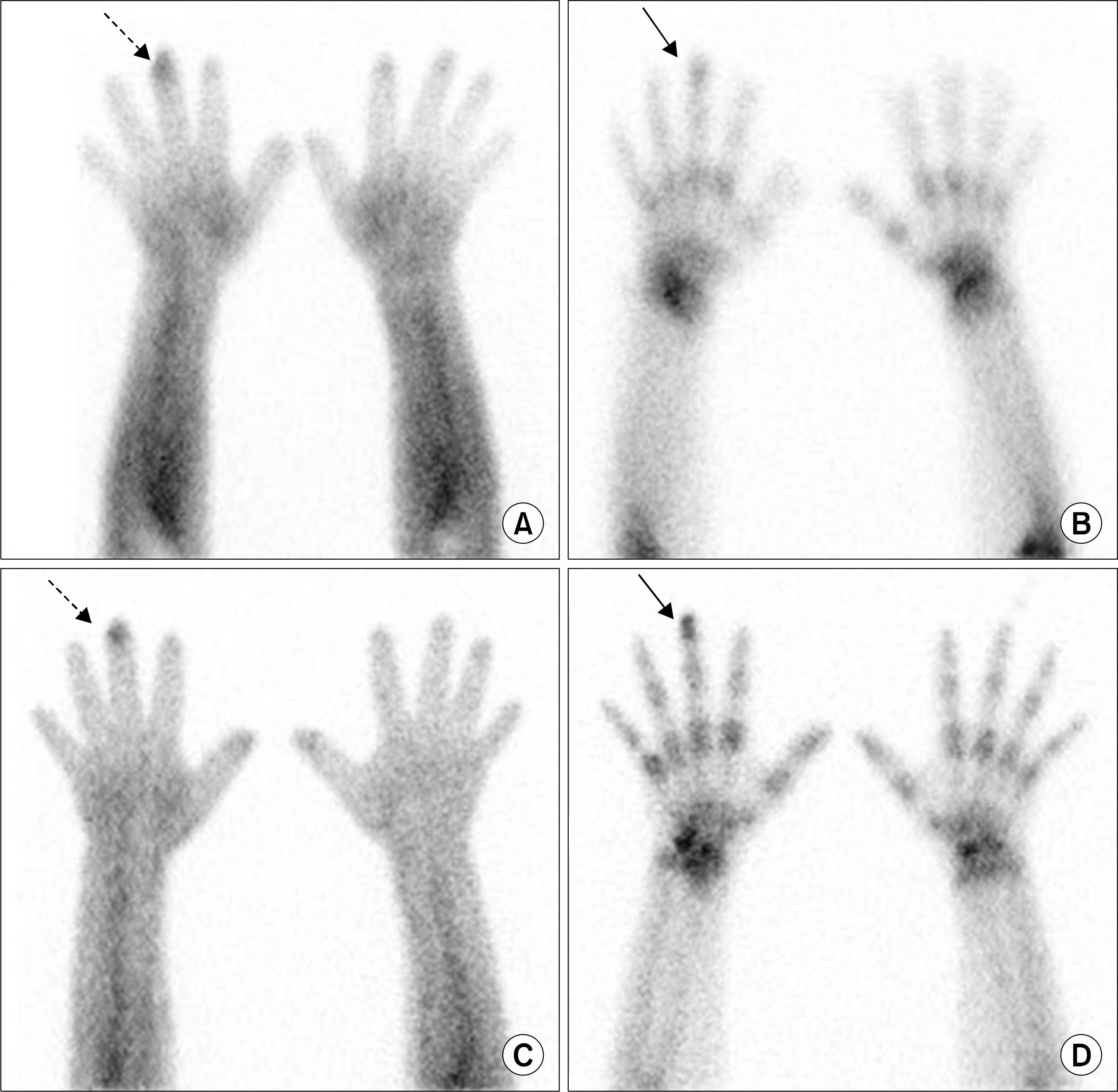
Figure 2. Three phase bone scan of both hands. (A, B) Blood pool activity and delayed 3-phase bone scan images at the time when the initial digital ulcer was noted. Localized increased blood pool activity was observed in the distal portion of the right third digit (A, dotted arrow). Minimally increased uptake was visible at the distal phalanx of the right third digit on the delayed image (B, arrow), which might have been caused by secondary hyperemia due to the soft tissue ulcer. (C, D) At the time of the 2-month follow-up 3-phase bone scan, the patient's symptoms were worsening. The localized blood pool activity of the right third digit was more intense (C, dotted arrow). At this time, prominent uptake was noted in the distal phalanx of the right third digit on the delayed image (D, arrow). This finding suggested the possibility of osteomyelitis of the distal phalanx of the right third digit.
Reference
-
1. Black CM, Matucci-Cerinic M, Guillevin L. Progress in systemic sclerosis: a 10-year perspective. Rheumatology (Oxford). 2009; 48(Suppl 3):iii1–2.
Article2. Herrick AL. Management of raynaud's phenomenon and digital ischemia. Curr Rheumatol Rep. 2013; 15:303.
Article3. Amanzi L, Braschi F, Fiori G, Galluccio F, Miniati I, Guiducci S, et al. Digital ulcers in scleroderma: staging, characteristics and sub-setting through observation of 1614 digital lesions. Rheumatology (Oxford). 2010; 49:1374–82.
Article4. Wigley FM. Vascular disease in scleroderma. Clin Rev Allergy Immunol. 2009; 36:150–75.
Article5. Silva I, Almeida J, Vasconcelos C. A PRISMA-driven systematic review for predictive risk factors of digital ulcers in systemic sclerosis patients. Autoimmun Rev. 2015; 14:140–52.
Article6. Harrison BJ, Silman AJ, Hider SL, Herrick AL. Cigarette smoking as a significant risk factor for digital vascular disease in patients with systemic sclerosis. Arthritis Rheum. 2002; 46:3312–6.
Article7. Chung L, Fiorentino D. Digital ulcers in patients with systemic sclerosis. Autoimmun Rev. 2006; 5:125–8.
Article8. Schiopu E, Impens AJ, Phillips K. Digital ischemia in scleroderma spectrum of diseases. Int J Rheumatol. 2010; 2010; 923743.
Article9. Baron M, Skrinskas G, Urowitz MB, Madras PN. Prostaglandin E1 therapy for digital ulcers in scleroderma. Can Med Assoc J. 1982; 126:42–5.10. Wigley FM, Seibold JR, Wise RA, McCloskey DA, Dole WP. Intravenous iloprost treatment of Raynaud's phenomenon and ischemic ulcers secondary to systemic sclerosis. J Rheumatol. 1992; 19:1407–14.11. Korn JH, Mayes M, Matucci Cerinic M, Rainisio M, Pope J, Hachulla E, et al. Digital ulcers in systemic sclerosis: prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum. 2004; 50:3985–93.
Article12. Matucci-Cerinic M, Denton CP, Furst DE, Mayes MD, Hsu VM, Carpentier P, et al. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2011; 70:32–8.
Article13. Agard C, Carpentier PH, Mouthon L, Clerson P, Gressin V, Bérezné A, et al. Use of bosentan for digital ulcers related to systemic sclerosis: a real-life retrospective French study of 89 patients treated since specific approval. Scand J Rheumatol. 2014; 43:398–402.
Article14. Tingey T, Shu J, Smuczek J, Pope J. Meta-analysis of healing and prevention of digital ulcers in systemic sclerosis. Arthritis Care Res (Hoboken). 2013; 65:1460–71.
Article15. Mayes MD. Endothelin and endothelin receptor antagonists in systemic rheumatic disease. Arthritis Rheum. 2003; 48:1190–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Systemic Lupus Erythematosus Diagnosed by Initial Presentation of Digital Gangrene
- A Case of Systemic Sclerosis Manifesting as Digital Finger Ulcers and Leg Ulcers
- A Case of Digital Ulcer in Systemic Sclerosis, Treated with Oral Sildenafil (Phosphodiesterase-5 Inhibitor, Viagra(R))
- A Case of Intractable Hiccups as Presenting Symptom of Multiple Sclerosis
- Improved Gastrointestinal Involvement in Systemic Sclerosis after Immunoglobulin Treatment
