J Korean Surg Soc.
2013 Nov;85(5):244-247.
Use of video-assisted thoracoscopic surgery to retrieve a broken guidewire
- Affiliations
-
- 1Department of Surgery, Bucheon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Bucheon, Korea. dosangs@catholic.ac.kr
Abstract
- Subclavian venous catheterization was once widely used for volume resuscitation, emergency venous access, chemotherapy, parenteral nutrition, and hemodialysis. However, its use has drastically reduced recently because of life-threatening complications such as hemothorax, pneumothorax. In this case, a patient admitted for a scheduled operation underwent right subclavian venous catheterization for preoperative, intraoperative, and postoperative volume resuscitation and parenteral nutrition. The procedure was performed by an experienced senior resident. Despite detecting slight resistance during the guidewire insertion, the resident continued the procedure to the point of being unable to advance or remove it, then attempted to forcefully remove the guidewire, but it broke and became entrapped within the thorax. We tried to remove the guidewire through infraclavicular skin incision but failed. So video-assisted thoracoscopic surgery was used to remove the broken guidewire. This incident demonstrates the risks of subclavian venous catheterization and the importance of using a proper and gentle technique.
Keyword
MeSH Terms
Figure
-

Fig. 1 The Spectrum Central Venous Catheter Set (length, 20 cm; size, 7.0 F; William A. Cook Australia Pty. Ltd.).

Fig. 2 J-shaped guide wire tip.
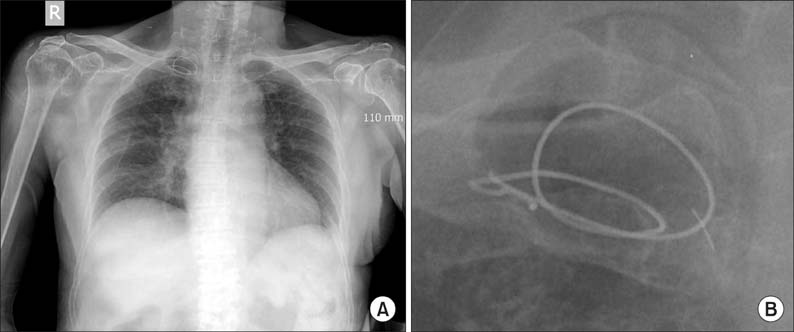
Fig. 3 (A) Chest radiography showed looped and entrapped guide wire. (B) Close up view of entrapped guide wire.

Fig. 4 Chest computed tomographic scan showed entrapped guide wire located outside the vein.
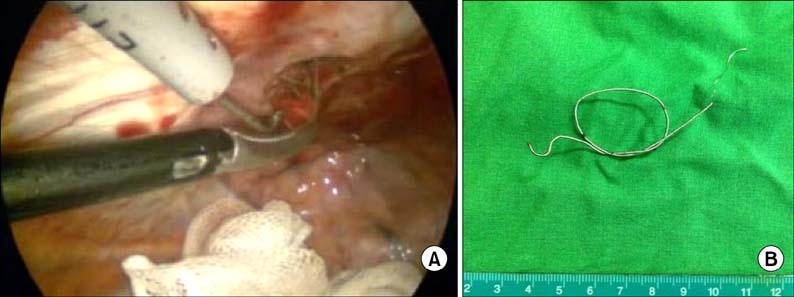
Fig. 5 (A) Entrapped guide wire visualized on thoracoscopy. (B) Completely removed guide wire.
Reference
-
1. De Moor B, Vanholder R, Ringoir S. Subclavian vein hemodialysis catheters: advantages and disadvantages. Artif Organs. 1994; 18:293–297.2. Emerman CL, Bellon EM, Lukens TW, May TE, Effron D. A prospective study of femoral versus subclavian vein catheterization during cardiac arrest. Ann Emerg Med. 1990; 19:26–30.3. Fragou M, Gravvanis A, Dimitriou V, Papalois A, Kouraklis G, Karabinis A, et al. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Crit Care Med. 2011; 39:1607–1612.4. Mansfield PF, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Complications and failures of subclavian-vein catheterization. N Engl J Med. 1994; 331:1735–1738.5. Slama M, Novara A, Safavian A, Ossart M, Safar M, Fagon JY. Improvement of internal jugular vein cannulation using an ultrasound-guided technique. Intensive Care Med. 1997; 23:916–919.6. Wang HE, Sweeney TA. Subclavian central venous catheterization complicated by guidewire looping and entrapment. J Emerg Med. 1999; 17:721–724.7. Onan B, Oz K, Onan IS. Knotted Seldinger guidewire as a complication of Hickman catheter implantation. J Vasc Access. 2010; 11:171–172.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Video assisted thoracoscopic surgery, 31 cases
- Video-assisted Thoracoscopic Surgery in Thoracic Surgical Field
- Video-assisted Thoracioscopic Surgery under Epidural Anesthesia in the High-Risk Patients with Secondary Spontaneous Pneumothorax
- Comparision of Clinical Results of Video-Assisted Thoracoscopic Surgery and Axillary Mini-Thoractomy for Spontaneous Pneumothorax
- Management of Complications During Video-Assisted Thoracic Surgery Lung Resection and Lymph Node Dissection
