Acute gastric volvulus treated with laparoscopic reduction and percutaneous endoscopic gastrostomy
- Affiliations
-
- 1Department of Surgery, Postgraduate School of Medicine, Gyeongsang National University, Jinju, Korea. yjleegnu@gmail.com
- 2Department of Internal Medicine, Postgraduate School of Medicine, Gyeongsang National University, Jinju, Korea.
- 3Gyeongnam Regional Cancer Center, Gyeongsang National University, Jinju, Korea.
- 4Institue of Health Sciences, Gyeongsang National University, Jinju, Korea.
Abstract
- Acute gastric volvulus requires emergency surgery, and a laparoscopic approach for both acute and chronic gastric volvulus was reported recently to give good results. The case of a 50-year-old patient with acute primary gastric volvulus who was treated by laparoscopic reduction and percutaneous endoscopic gastrostomy is described here. This approach seems to be feasible and safe for not only chronic gastric volvulus, but also acute gastric volvulus.
Figure
-

Fig. 1 The simple abdominal X-ray and endoscopic images at presentation. (A) X-ray image in the abdominal erect view showing the distention and air-fluid levels in the stomach. (B) X-ray image in the supine view showing the distended and mass-like lesion in the epigastric area. (C) Endoscopic image showing the congested and edematous gastric wall.

Fig. 2 Schematic depiction of the gastric volvulus of the patient and preoperative abdominal computed tomography (CT) images in the coronal view. (A) The stomach had rotated (gray arrow) along the axis (dot line) joining the mid and lesser curvatures (mesentero-axial volvulus). The meaning of arrows 1, 2, and 3 are indicated in the legends of Fig. 2B and 2C. (B) CT image. Arrow ① indicates the esophagus and gastroesophageal junction, while arrow ② shows the body portion is superior to the fundus area. (C) CT image. Arrow ③ shows the gastric low body is located below the diaphragm and is connected to the duodenum.
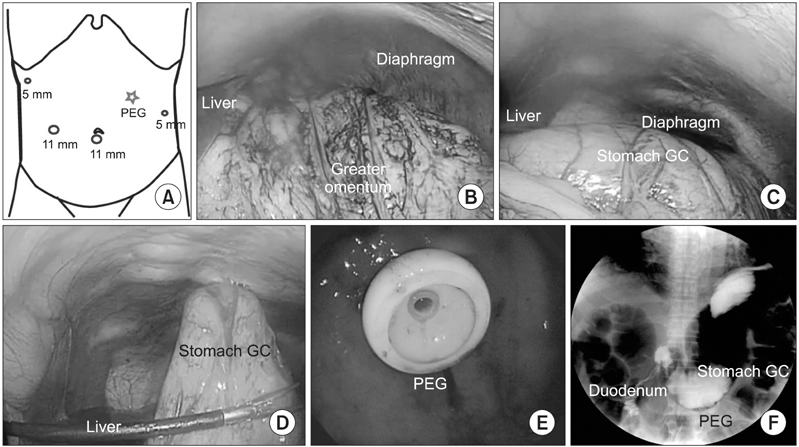
Fig. 3 Intraoperative findings and postoperative upper gastrointerstinal study. (A) Depiction of the abdomen showing the placement of the four trocars (marked by circles; two 11-mm and two 5-mm ports). The position of the percutaneous endoscopic gastrostomy (PEG) is shown by the red star. (B) Before the reduction, blood stains were observed in the greater omentum along with a mass-like twisted stomach below the diaphragm. (C) After the reduction, normal stomach anatomy was observed. (D) Laparoscopic view of the PEG that had been inserted in the midbody greater curvature side. (E) Endoscopic view of the inserted PEG. (F) The postoperative upper gastrointestinal contrast study confirmed complete reduction of the stomach and the absence of evidence of obstruction. GC, greater curvature.
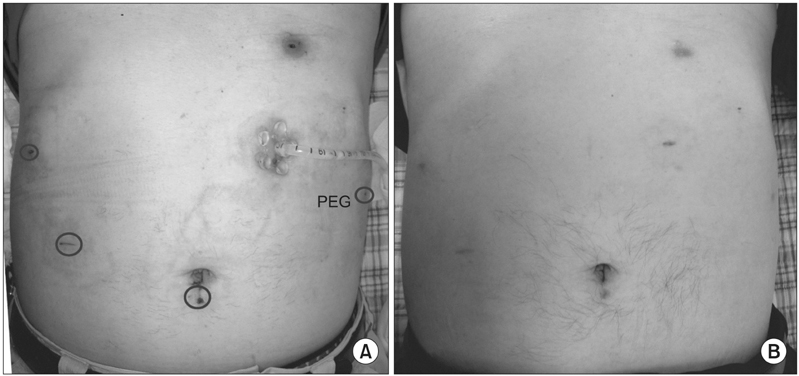
Fig. 4 Photos of the postoperative wounds. (A) On the fourteenth postoperative day, the percutaneous endoscopic gastrostomy (PEG) was still inserted. The port site wounds are indicated by blue circles. (B) The abdomen 5 months after the initial operation.
Reference
-
1. Tanner NC. Chronic and recurrent volvulus of the stomach with late results of "colonic displacement". Am J Surg. 1968. 115:505–515.2. Carter R, Brewer LA 3rd, Hinshaw DB. Acute gastric volvulus: a study of 25 cases. Am J Surg. 1980. 140:99–106.3. Wasselle JA, Norman J. Acute gastric volvulus: pathogenesis, diagnosis, and treatment. Am J Gastroenterol. 1993. 88:1780–1784.4. Naim HJ, Smith R, Gorecki PJ. Emergent laparoscopic reduction of acute gastric volvulus with anterior gastropexy. Surg Laparosc Endosc Percutan Tech. 2003. 13:389–391.5. Umehara Y, Kimura T, Okubo T, Sano Y, Ori T, Sakamoto R, et al. Laparoscopic gastropexy in a patient with chronic gastric volvulus. Surg Laparosc Endosc. 1992. 2:261–264.6. Eckhauser ML, Ferron JP. The use of dual percutaneous endoscopic gastrostomy (DPEG) in the management of chronic intermittent gastric volvulus. Gastrointest Endosc. 1985. 31:340–342.7. Katkhouda N, Mavor E, Achanta K, Friedlander MH, Grant SW, Essani R, et al. Laparoscopic repair of chronic intrathoracic gastric volvulus. Surgery. 2000. 128:784–790.8. Cybulsky I, Himal HS. Gastric volvulus within the foramen of Morgagni. Can Med Assoc J. 1985. 133:209–210.9. Luketich JD, Raja S, Fernando HC, Campbell W, Christie NA, Buenaventura PO, et al. Laparoscopic repair of giant paraesophageal hernia: 100 consecutive cases. Ann Surg. 2000. 232:608–618.10. Palanivelu C, Rangarajan M, Shetty AR, Senthilkumar R. Laparoscopic suture gastropexy for gastric volvulus: a report of 14 cases. Surg Endosc. 2007. 21:863–866.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Management of Sigmoid Volvulus for Which Endoscopic Reduction had Failed
- A Case of Gastric Volvulus Reduced by Endoscope
- A Case of Mesenteroaxial Gastric Volvulus Diagnosed Using Endoscopic Procedure
- Chronic Gastric Volvulus with Laparoscopic Gastropexy after Endoscopic Reduction: A Case Report
- A Case of Percutaneous Endoscopic Gastrostomy in a Patient with Liver Cirrhosis Accompanied by Both Esophageal and Gastric Varices
