Diffuse Idiopathic Skeletal Hyperostosis Associated with Dysphonia and Dysphagia: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, National Police Hospital, Seoul, Korea. hsh@nph.go.kr
Abstract
- We encountered a rare case of diffuse idiopathic skeletal hyperostosis (DISH) associated with dysphonia and dysphagia. An 80 year-old man developed progressive dysphonia and dysphagia. The radiology study, esophagogram and nasopharyngoscopic exam revealed the esophagus and the posterior wall of the nasopharynx to be severely compressed by the unfused osteophyte of the 3rd and 4th cervical intervertebral space. It was thought that the osteophyte formation was caused by not merely DISH but degenerative changes due to a concentration of stress around the unfused hyperostosis. A resection of the osteophyte was performed, which resolved the clinical symptoms. The follow-up radiology study, esophagogram and nasopharyngoscopic exam showed that the osteophyte had disappeared.
MeSH Terms
Figure
-
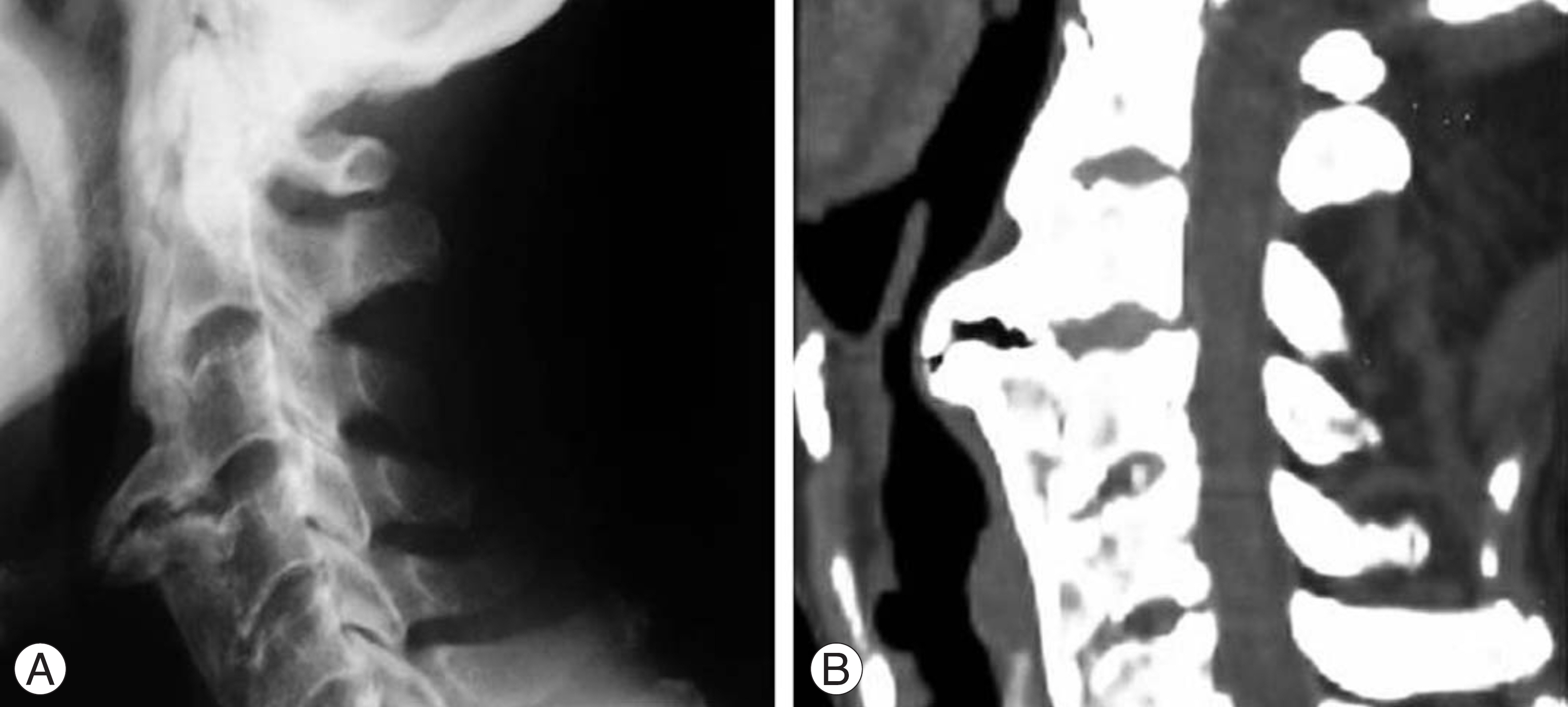
Fig. 1. (A) and (B) Preoperative cervical spine lateral radiograph and sagittal CT scan show contiguous ossification along the anterior aspect of the first (C1) to seventh cervical vertebrae (C7), with a localized osteophyte between C3 and C4.
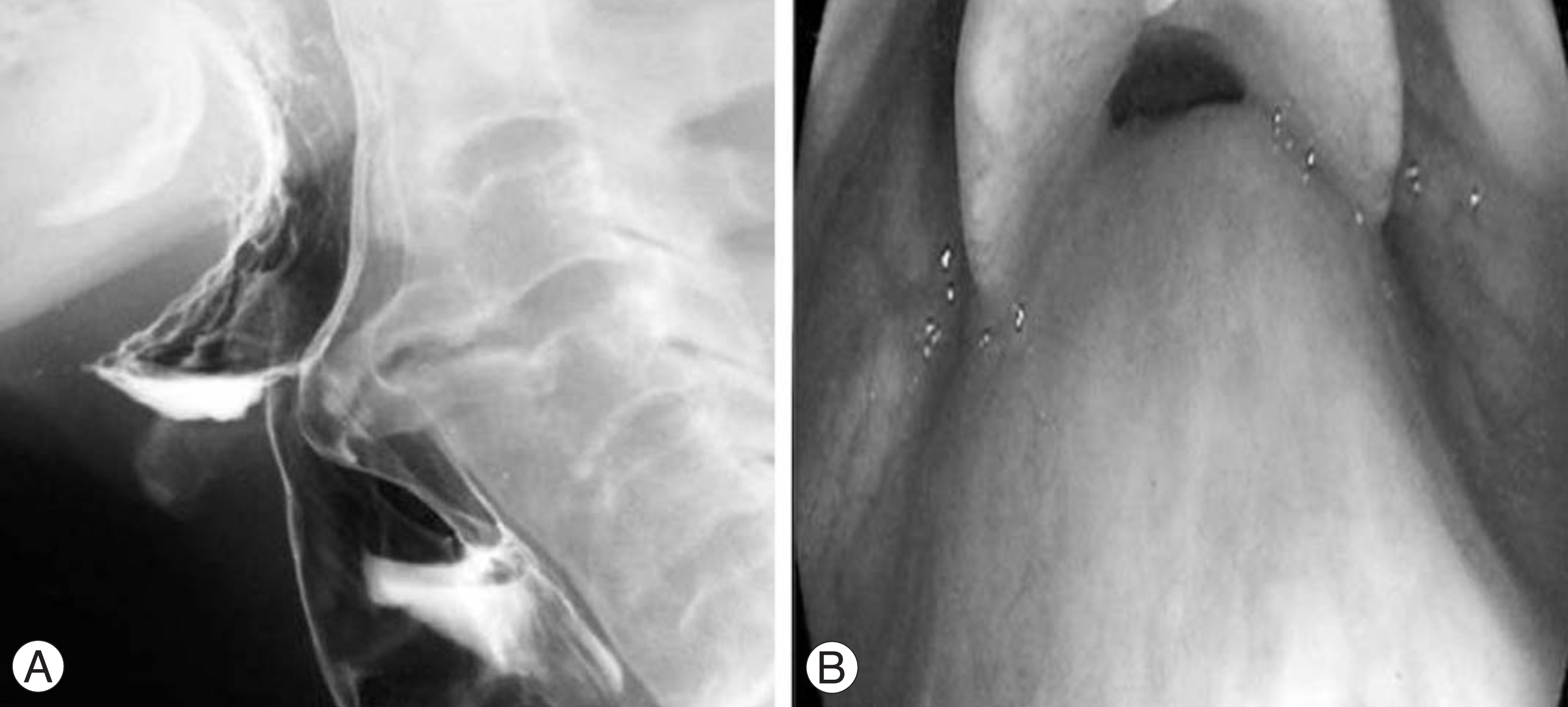
Fig. 2. (A) In barium esophagogram, the posterior wall of the hypopharynx is indented by osteophytes and the esophagus is significantly narrowed from C3 to C4. (B) Nasopharyngoscopic view shows mass projecting from posterior wall of hypopharynx.

Fig. 3. (A) and (B) Postoperative cervical spine lateral radiograph and sagittal CT scan show no osteophytes between C3 and C4.
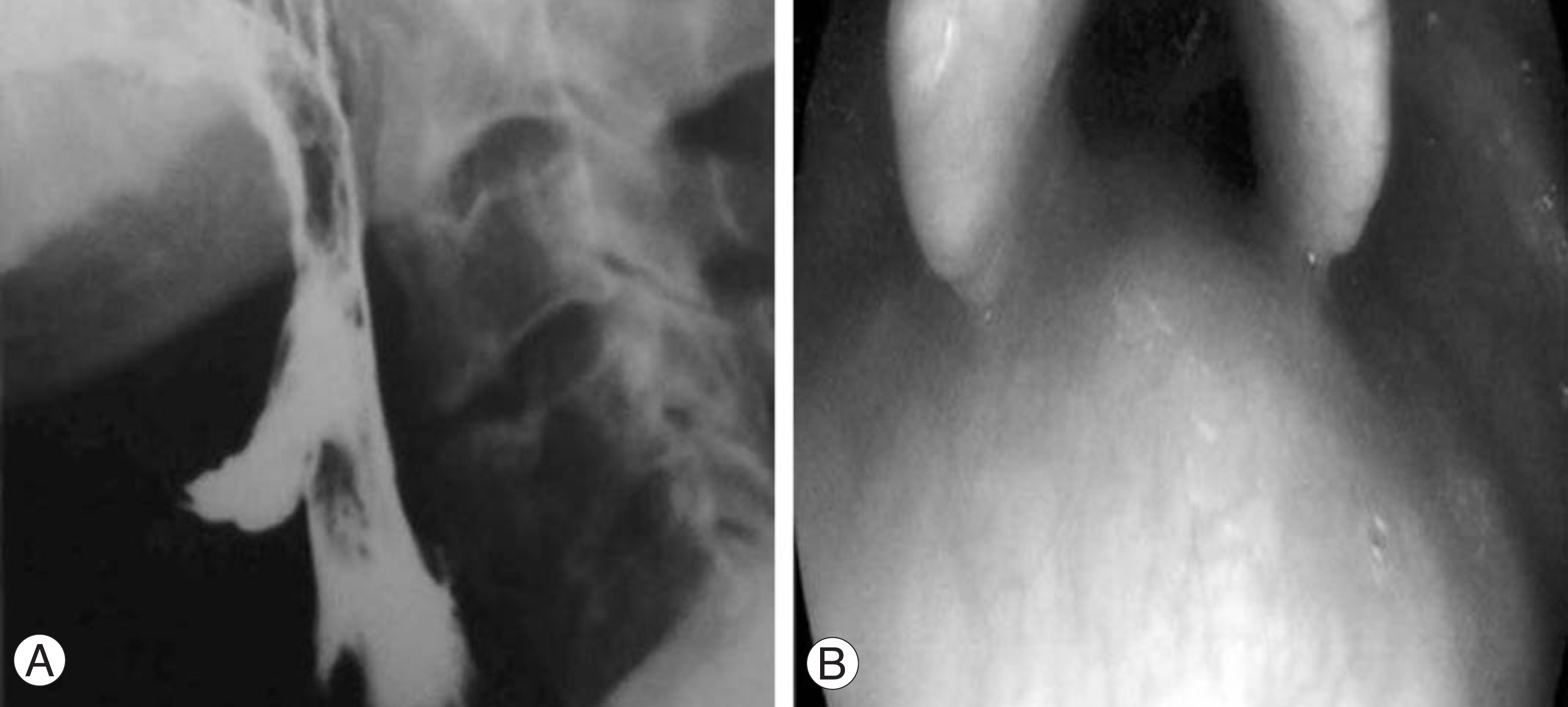
Fig. 4. (A) In barium esophagogram, no osteophytes are seen impinging on the posterior wall of the pharynx and contrast media pass-es well through the esophagus. (B) Nasopharyngoscopic view shows widened pharynx without mass.
Reference
-
1). Resnick D, Shapiro RF, Wiesner KB, Niwayama G, Utsinger PD, Shaul SR. Diffuse idiopathic hyperostosis. Semin Arthritis Rheum. 1978; 7:153–187.2). Forestier J, Rotes-Querol J. Senile ankylosing hyperostosis of the spine. Ann Rheum Dis. 1950; 9:321–330.
Article3). Resnick D, Shaul SR, Robins JM. Diffuse idiopathic skeletal hyperostosis (DISH). Forestier's disease with extraspinal manifestations. Diagnostic Radiology. 1975; 115:513–524.
Article4). Weinfeld RM, Olson PN, Maki DD, Griffiths HJ. The prevalence of diffuse idiopathic skeletal hyperostosis (DISH) in two large American Midwest metropolitan hospital populations. Skeletal Radiol. 1997; 26:222–225.
Article5). Kim SK, Choi BR, Kim CG, et al. The prevalence of diffuse idiopathic skeletal hyperostosis in Korea. J Rheumatol. 2004; 31:2032–2035.6). Gamach FW, Voorhies RM. Hypertrophic cervical osteophytes causing dysphagia. A review. J Neurosurgery. 1980; 53:338–343.7). Kim YW, Jang HG, Jung JC, Lee KB. Dysphagia due to diffuse idiopathic skeletal hyperostosis of the cervical spine. J Kor Soc Spine Surg. 2003; 10:335–339.8). Papakostas K, Thakar A, Nandapalan V, O'Sullivan G. An unusual case of stridor due to osteophytes of the cervical spine (Forestier's disease). J Laryngol Otol. 1999; 113:65–67.
Article9). Karlins NL, Yagan R. Dyspnea and hoarseness: A complication of diffuse idiopathic skeletal hyperostosis. Spine. 1991; 16:235–237.
Article10). Eviatar E, Harell M. Diffuse idiopathic skeletal hyperostosis with dysphagia (A review). J Laryngol Otol. 1987; 101:627–632.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dysphagia due to Cervical Osteophytes: Case Report
- Dysphagia Due to Diffuse Idiopathic Skeletal Hyperostosis of The Cervical Spine: A Case Report
- A Case of Dysphagia due to Cricopharyngeal Dysfunction and Diffuse Idiopathic Skeletal Hyperostosis
- A Case of Diffuse Idiopathic Skeletal Hyperostosis with Dysphagia
- A Case of Forestier's Disease with Dyspnea
