Thoracic Myelopathy due to Thoracolumbar Kyphosis and Spinal Stenosis in Achondroplasia: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. amhangpark@yahoo.co.kr
Abstract
- Achondroplasia is abnormal intracartilagenous ossification that's caused by a genetic point mutation. Thoracic myelopathy in achondroplasia that is due to thoracolumbar kyphosis and spinal stenosis is a rare finding. There is no report available on this topic in Korea. We report here a case of achondroplasia with thoracic myelopathy due to thoracolumbar kyphosis and spinal stenosis, and we include a brief review of literature.
Figure
-

Fig. 1, 2. The simple radiography of spine anteroposterior and lateral view in preoperative state. T12 vertebral body is wedge shape and vertebral Cobb’s angle is 83 degree at level of thoracolumbar junction. Sagittal vertebral axis(SVA) is positive about 4cm in lateral view. Lumbar hyperlordosis coexist with scoliosis and deformity of thoracolumbar spine.

Fig. 3. Preoperative MRI (A) T1 Sagittal image, (B) T2 Sagittal image, (C) T2 Axial image(T 11- T12 disc level),(D) T2 Axial image(T12- L1 disc level) There is central spinal stenosis at the level of T11/12, T12/L1 and central spinal stenosis, with bulging disc at the level of L2/3, L3/4, L4/5. The shape of T12 vertebral body is wedge form and short pedicles with bilateral neural foraminal narrowing coexist at lumbar and lower thoracic spines.
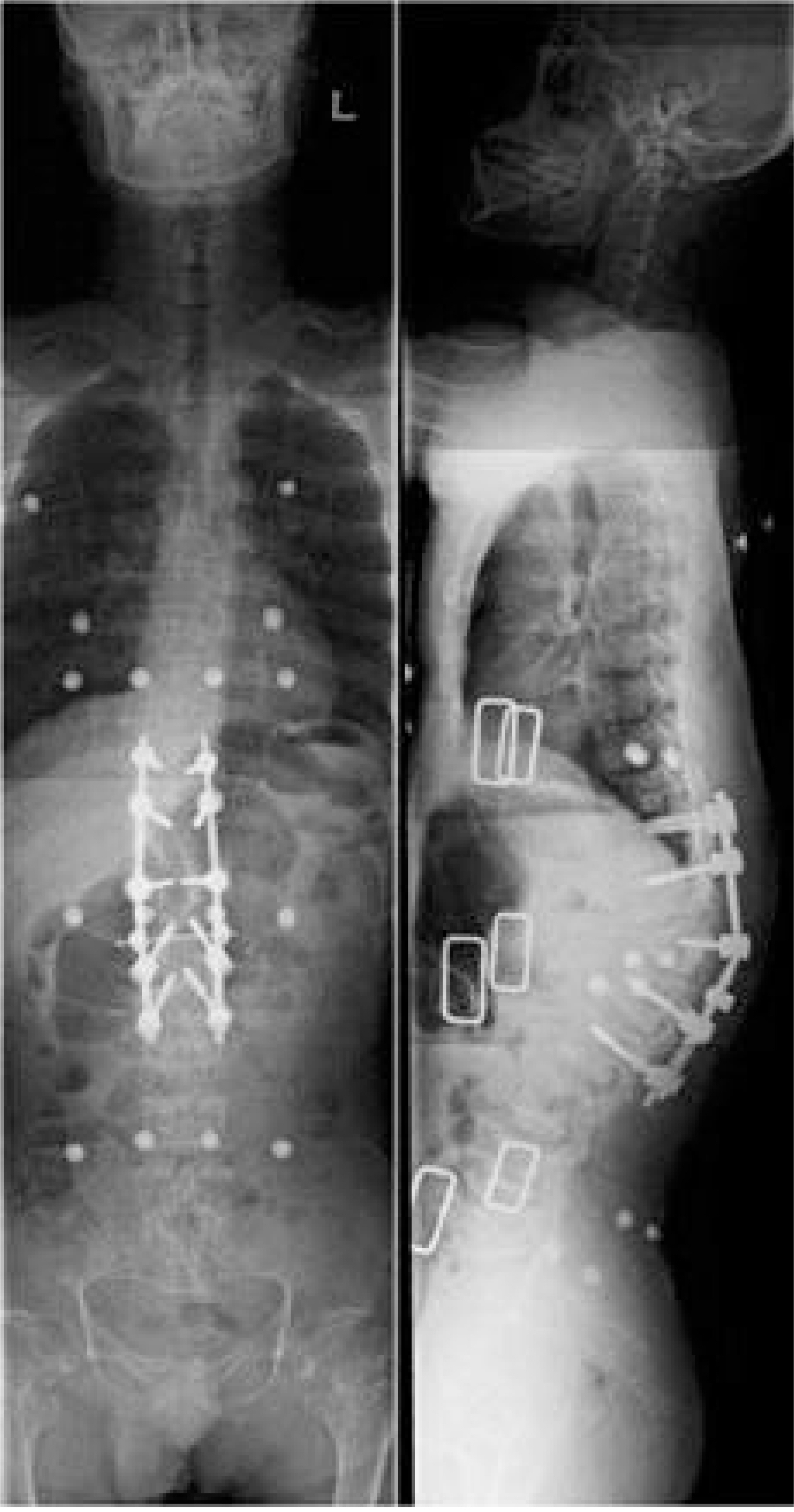
Fig. 4. The simple radiography of whole spine anteroposterior and lateral view in postoperative state. The Cobb’s angle is decreased to 52 degree at level of thoracolumbar junction. Sagittal vertebral axis(SVA) is corrected to negative 3.6 cm which from posterosuperior corner of S1.

Fig. 5. The follow up simple radiography of whole spine anteroposterior and lateral view at 6 months after operation. Cobb’s angle is 50 degree and neurologic symptoms are subsided.
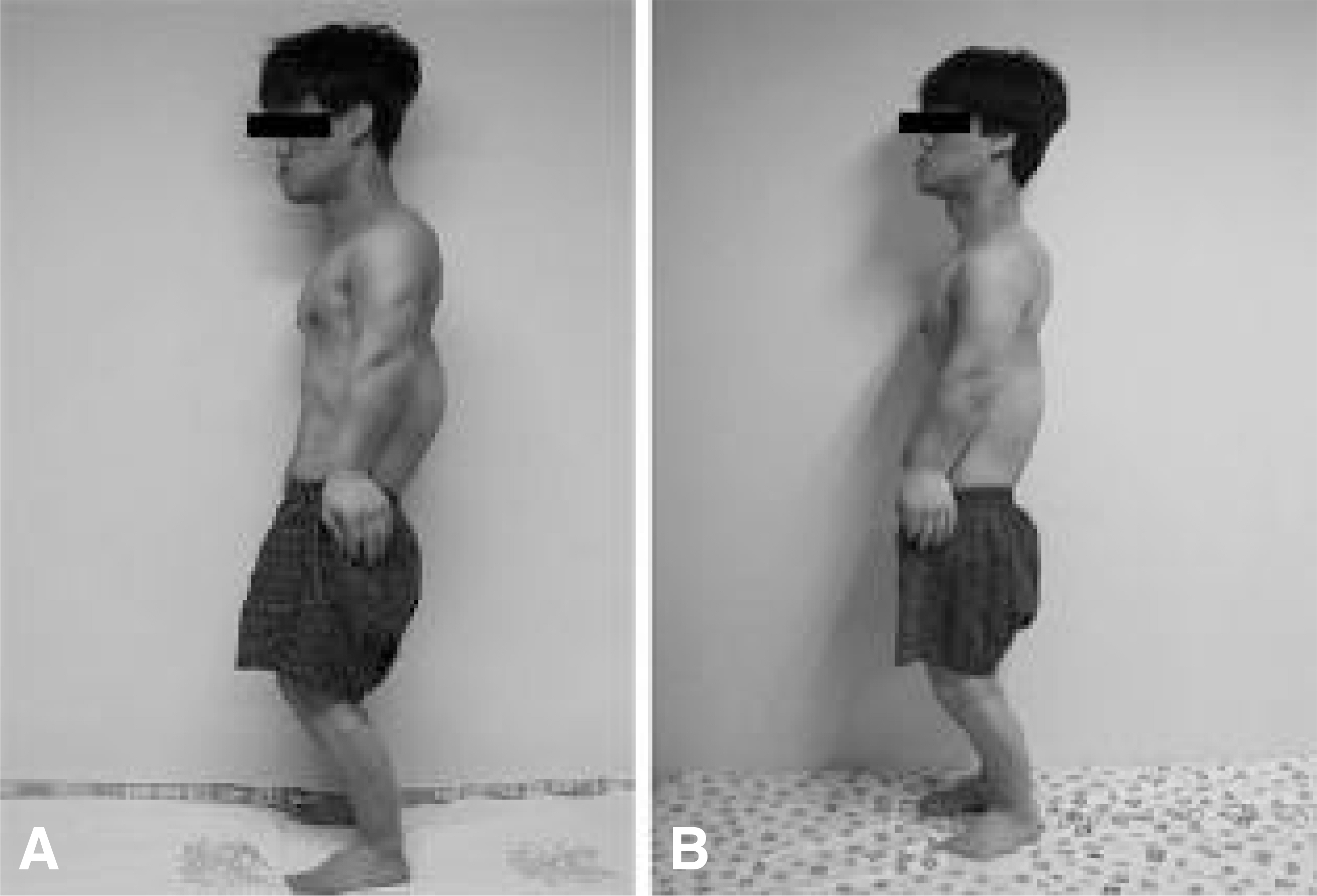
Fig. 6. The photography which compared the preoperative state(A) with the postoperative state(B). Back deformity and positional impairment are improved.
Reference
-
1). Fortuna A, Ferrante L, Acqui M, Santoro A, Mastronardi L. Narrowing of thoracolumbar spinal canal in achondroplasia. J Neurosurgical science. 233:185–196. 1989.2). Kahanovitz N, Rimoin DL, Sillence DO. The clinical spectrum of lumbar spine disease in achondroplasia. Spine. 7:137–140. 1982.
Article3). Kopits SE. Thoracolumbar kyphosis and lumbosacral hyperlordosis in achondroplastic children. Basic Life Sci. 48:241–255. 1988.
Article4). Pauli RM, Breed A, Horton VK, et al. Prevention of fixed, angular kyphosis in achondroplasia. J Pediatr Orthop. 17:726–733. 1997.
Article5). Sanjay NM, Howard WM. Thoracolumbar Spinal deformity in Achondroplasia. Neurosurg Focus. 14(1):1–8. 2003.6). Shikata J, Yamamuro T, Iida H, et al. Surgical treat - ment of achondroplastic dwarfs with paraplegia. Surg Neurol. 29:125–130. 1988.7). Thomeer RT, van Dijk JM. Surgical treatment of lumbar stenosis in achondroplasia. J Neurosurg. 96(Spine 3):292–297. 2002.
Article8). Tolo VT. Spinal deformity in short-stature syndromes. Instr Course Lect. 39:399–405. 1990.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Spinal Stenosis Secondary to Achondroplasia
- Aneurysmal Subarachnoid Hemorrhage Associated with Achondroplasia: Case Report
- A Case of Thoracic Spinal Canal Stenosis
- Thoracic Disc Herniation of the Adjacent Segment With Acutely Progressing Myelopathy
- Traumatic Cauda Equina Syndrome Due to Spinal Stenosis in an Achondroplastic Patient: A Case Report
