Intracranial Extra-Axial Ependymoma in the Ambient Cistern That Initially Presented as Calcification: A Report of Case
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. flightdr61@cau.ac.kr
- 2Department of Neurosurgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
Abstract
- Ependymomas usually occur in intraventricular or intraspinal locations. Intracranial extraaxial ependymomas (IEAEs) are very rare. Here, we present an unusual case of an IEAE in 25-year-old man. The patient experienced head trauma two and half years prior to presentation, at which time brain computed tomography (CT) showed only a dense calcification in the left ambient cistern. After two and a half years, follow up brain CT and magnetic resonance imaging depicted interval growth of a calcified mass with cystic change. The tumor was successfully treated surgically, and the pathologic examination confirmed ependymoma.
Figure
-
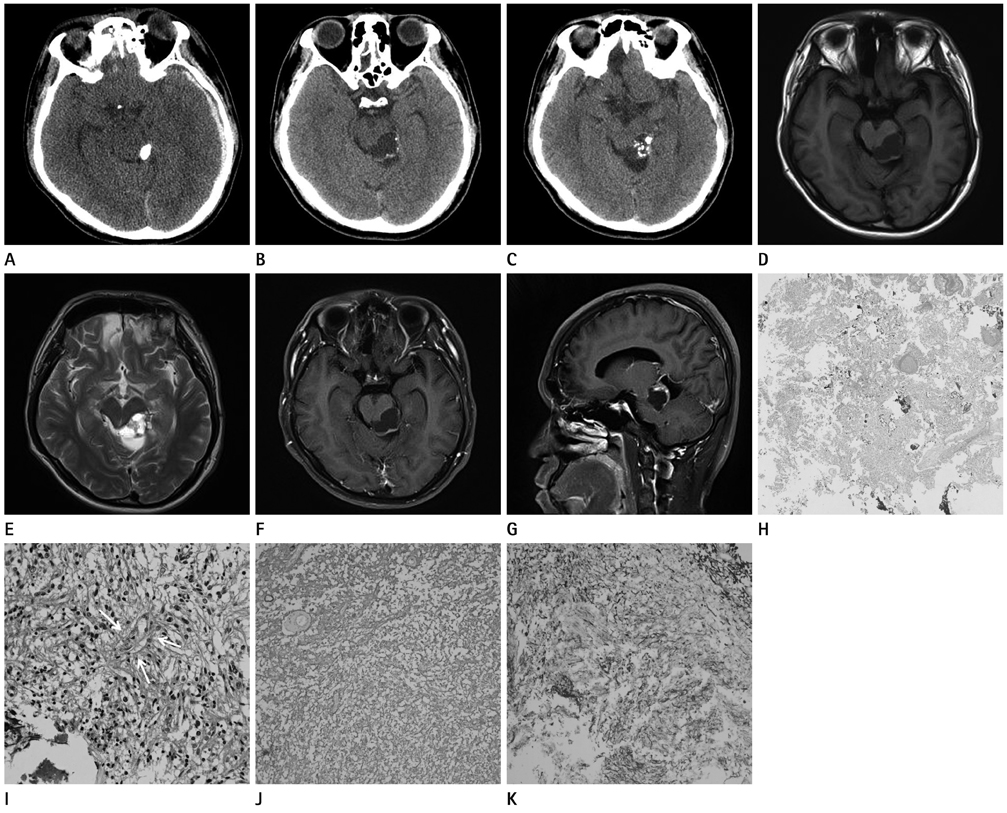
Fig. 1 A 25-year-old man with an intracranial extraaxial ependymoma in left ambient cistern. A. Nonenhanced CT shows a dense, large (1.2 × 0.8 cm) calcification in the left ambient cistern. B, C. Nonenhanced CT shows a lobulated (2.5 × 2.0 cm) cystic mass (B) with fragmented calcifications (C) in the left ambient cistern. D-G. An axial T1 weighted image shows a lobulated hypointense mass with a peripheral thin solid component in the left ambient cistern (D). An axial T2 weighted image shows a hyperintense mass with low signal multiple dot calcifications (E). Axial (F) and sagittal (G) gadolinium enhanced T1-weighted images show heterogeneous enhancement in the solid component of the mass. H, I. A low-power photomicrograph (hematoxylin and eosin, × 40) shows that the tumor has moderate cellularity and numerous calcifications (H). A high-power photomicrograph (hematoxylin and eosin, × 400) shows sheets of spindled or ephithelioid cells with round to oval nuclei in the tumor. A nuclear free zone is seen around the central blood vessel (pseudorosette; white arrows) (I). J, K. Immunohistochemical examination of the tumor reveals that S-100 (J) and glial fibrillary acid protein (K) stains are positive (× 200).
Reference
-
1. Rezai AR, Woo HH, Lee M, Cohen H, Zagzag D, Epstein FJ. Disseminated ependymomas of the central nervous system. J Neurosurg. 1996. 85:618–624.2. Armington WG, Osborn AG, Cubberley DA, Harnsberger HR, Boyer R, Naidich TP, et al. Supratentorial ependymoma: CT appearance. Radiology. 1985. 157:367–372.3. Choi JY, Chang KH, Yu IK, Kim KH, Kwon BJ, Han MH, et al. Intracranial and spinal ependymomas: review of MR images in 61 patients. Korean J Radiol. 2002. 3:219–228.4. Fukui MB, Hogg JP, Martinez AJ. Extraaxial ependymoma of the posterior fossa. AJNR Am J Neuroradiol. 1997. 18:1179–1181.5. Donich D, Lee JH, Prayson R. Giant extra-axial cerebellopontine angle/cavernous sinus ependymoma: case report. Neurosurgery. 1999. 44:195–198.6. Little NS, Morgan MK, Eckstein RP. Primary ependymoma of a cranial nerve. Case report. J Neurosurg. 1994. 81:792–794.7. Hayashi K, Tamura M, Shimozuru T, Kasamo S, Hirahara K, Kadota K, et al. Extra-axial ependymoma--case report. Neurol Med Chir (Tokyo). 1994. 34:295–299.8. Lyons MK, Kelly PJ. Posterior fossa ependymomas: report of 30 cases and review of the literature. Neurosurgery. 1991. 28:659–664. discussion 664-665.9. Hanchey RE, Stears JC, Lehman RA, Norenberg MD. Interhemispheric ependymoma mimicking falx meningioma. Case report. J Neurosurg. 1976. 45:108–112.10. Ozawa N, Nakayama K, Ohata K, Okamura T, Inoue Y. Tentorial schwannoma: a case report. Br J Radiol. 2003. 76:421–424.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supratentorial Anaplastic Ependymoma Mimicking an Extra-Axial Tumor: A Case Report
- A Case of Supratentorial Intra-axial Ependymoma Showing Exophytic Growth
- Gangliocytoma Mimicking Extra-axial Tumor: A Report of Two Cases
- Extra-Axial Medulloblastoma in the Cerebellar Hemisphere
- Extra-Axial and Clear Cell Type Ependymoma, Mimicking a Convexity Meningioma
