A Case of Statin-Induced Interstitial Pneumonitis due to Rosuvastatin
- Affiliations
-
- 1Department of Internal Medicine, The Armed Forces Medical Hospital, Seongnam, Korea. chrisjinny@naver.com
- 2Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 2320657
- DOI: http://doi.org/10.4046/trd.2015.78.3.281
Abstract
- Statins lower the hyperlipidemia and reduce the incidence of cardiovascular events and related mortality. A 60-year-old man who was diagnosed with a transient ischemic attack was started on acetyl-L-carnitine, cilostazol, and rosuvastatin. After rosuvastatin treatment for 4 weeks, the patient presented with sudden onset fever, cough, and dyspnea. His symptoms were aggravated despite empirical antibiotic treatment. All infectious pathogens were excluded based on results of culture and polymerase chain reaction of the bronchoscopic wash specimens. Chest radiography showed diffuse ground-glass opacities in both lungs, along with several subpleural ground-glass opacity nodules; and a foamy alveolar macrophage appearance was confirmed on bronchoalveolar lavage. We suspected rosuvastatin-induced lung injury, discontinued rosuvastatin and initiated prednisolone 1 mg/kg tapered over 2weeks. After initiating steroid therapy, his symptoms and radiologic findings significantly improved. We suggest that clinicians should be aware of the potential for rosuvastatin-induced lung injury.
MeSH Terms
-
Acetylcarnitine
Bronchoalveolar Lavage
Chemically-Induced Disorders
Cough
Dyspnea
Fever
Humans
Hydroxymethylglutaryl-CoA Reductase Inhibitors
Hyperlipidemias
Incidence
Ischemic Attack, Transient
Lung
Lung Diseases, Interstitial*
Lung Injury
Macrophages, Alveolar
Middle Aged
Mortality
Polymerase Chain Reaction
Prednisolone
Radiography
Thorax
Rosuvastatin Calcium
Acetylcarnitine
Prednisolone
Figure
-

Figure 1 (A-E) Chest radiography showed subtle diffuse ground glass opacity in both lower lobe field and subsegmental atelectasis in left lower lobe field on admission. A computed tomography scan of the chest showed diffuse ill-defined ground glass opacity with septal line thickening in bilateral lung fields combined with several subpleural ground glass opacity nodules on admission.
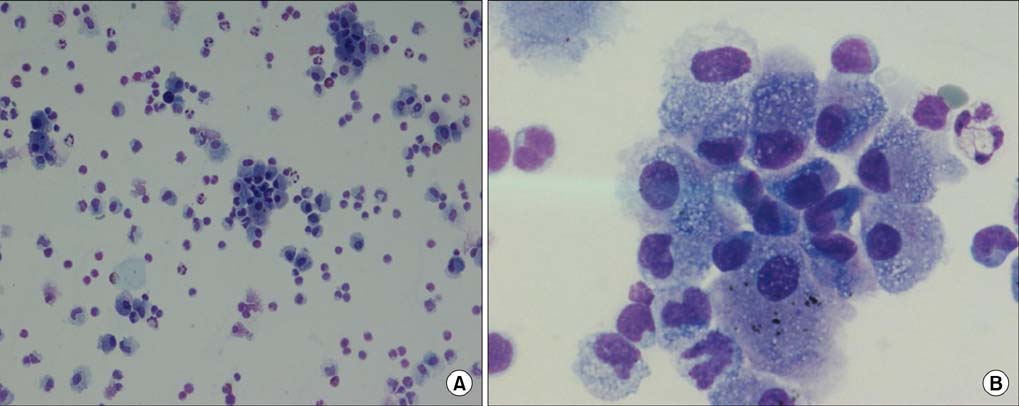
Figure 2 (A, B) H&E stained smear of bronchoalveolar lavage fluid showed a foamy appearance of the majority of alveolar macrophages (A, ×40; B, ×100).
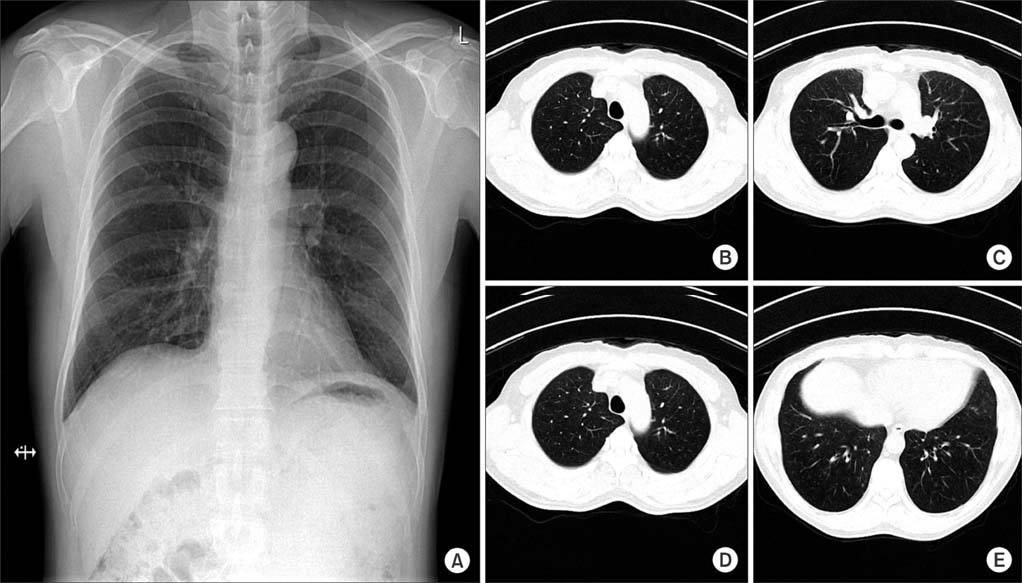
Figure 3 (A-E) Day 14 after initiation of steroid therapy, chest radiography showed disappearance of the previously noted diffuse ground-glass opacities in both lung fields. There were no other remarkable findings.
Reference
-
1. Rosenson RS, Tangney CC. Antiatherothrombotic properties of statins: implications for cardiovascular event reduction. JAMA. 1998; 279:1643–1650.2. Bellosta S, Paoletti R, Corsini A. Safety of statins: focus on clinical pharmacokinetics and drug interactions. Circulation. 2004; 109:23 Suppl 1. III50–III57.3. Alsheikh-Ali AA, Ambrose MS, Kuvin JT, Karas RH. The safety of rosuvastatin as used in common clinical practice: a postmarketing analysis. Circulation. 2005; 111:3051–3057.4. Hill C, Zeitz C, Kirkham B. Dermatomyositis with lung involvement in a patient treated with simvastatin. Aust N Z J Med. 1995; 25:745–746.5. Liebhaber MI, Wright RS, Gelberg HJ, Dyer Z, Kupperman JL. Polymyalgia, hypersensitivity pneumonitis and other reactions in patients receiving HMG-CoA reductase inhibitors: a report of ten cases. Chest. 1999; 115:886–889.6. Veyrac G, Cellerin L, Jolliet P. A case of interstitial lung disease with atorvastatin (Tahor) and a review of the literature about these effects observed under statins. Therapie. 2006; 61:57–67.7. Fernandez AB, Karas RH, Alsheikh-Ali AA, Thompson PD. Statins and interstitial lung disease: a systematic review of the literature and of food and drug administration adverse event reports. Chest. 2008; 134:824–830.8. Huang LK, Tsai MJ, Tsai HC, Chao HS, Lin FC, Chang SC. Statin-induced lung injury: diagnostic clue and outcome. Postgrad Med J. 2013; 89:14–19.9. Matsuno O. Drug-induced interstitial lung disease: mechanisms and best diagnostic approaches. Respir Res. 2012; 13:39.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Everolimus-Induced Interstitial Pneumonitis in a Patient with Metastatic Renal Cell Carcinoma: a Case Report
- Rosuvastatin-induced Generalized Drug Eruption
- A case of rifampicin-induced interstitial pneumonitis
- Successful Treatment of Interstitial Pneumonitis Induced by Leflunomide
- A Case of Nonspecific Interstitial Pneumonitis Improved After Cyclosporin Therapy
