Silicone Stent Placement for Primary Tracheal Amyloidosis Accompanied by Cartilage Destruction
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hjk3425@skku.edu
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Abstract
- Primary tracheal amyloidosis (PTA) can lead to airway obstructions, and patients with severe PTA should undergo bronchoscopic interventions in order to maintain airway patency. Focal airway involvements with amyloidosis can only be treated with mechanical dilatation. However, the PTA with diffused airway involvements and concomitant cartilage destructions requires stent placement. Limited information regarding the usefulness of silicone stents in patients with PTA has been released. Therefore, we report a case of diffused PTA with tracheomalacia causing severe cartilage destruction, which is being successfully managed with bronchoscopic interventions and silicone stent placements.
Keyword
MeSH Terms
Figure
-

Figure 1 Initial computed tomography (CT) and bronchoscopic findings with primary tracheal amyloidosis. (A) On the chest CT scan, the mid-trachea was narrowed to ~3 mm (black arrow) with irregular thickening of the wall and destructions of the tracheal cartilage (white arrows). (B) On bronchoscopy, diffused luminal narrowing secondary to submucosal infiltration was found from the level of thoracic inlet to the lower trachea.
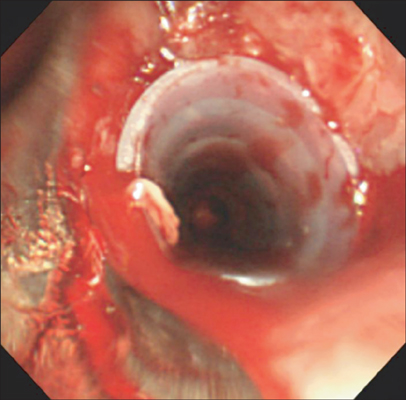
Figure 2 Silicone stent implantation in a patient with primary tracheal amyloidosis. A silicone airway stent (outer diameter 12 mm, inner diameter 10 mm, length 50 mm) was inserted into the trachea to maintain airway patency.
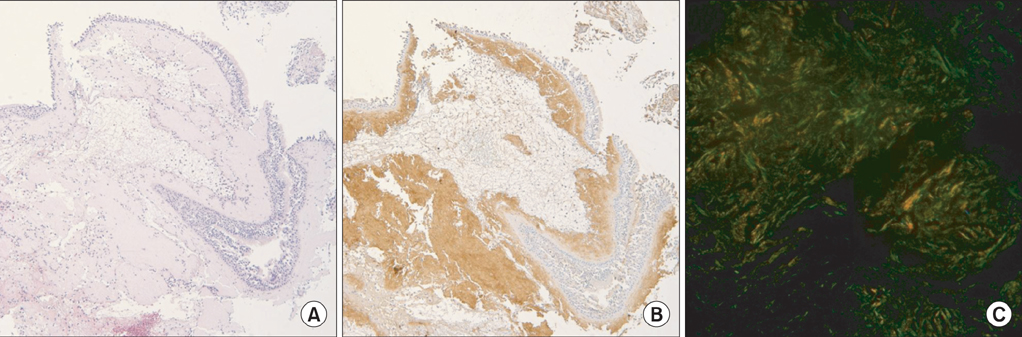
Figure 3 Histological examinations of the bronchoscopic biopsy. (A) There is a homogenous pink amorphous material in the subepithelial region (H&E stain, ×100). (B) The subepithelial amorphous material shows reactivities with the amyloid P stain (amyloid P stain, ×100). (C) Congo Red staining reveals apple-green birefringence under the polarized light (Congo Red, ×200).
Reference
-
1. Gillmore JD, Hawkins PN. Amyloidosis and the respiratory tract. Thorax. 1999; 54:444–451.2. Piazza C, Cavaliere S, Foccoli P, Toninelli C, Bolzoni A, Peretti G. Endoscopic management of laryngo-tracheobronchial amyloidosis: a series of 32 patients. Eur Arch Otorhinolaryngol. 2003; 260:349–354.3. Ryu YJ, Kim H, Yu CM, Choi JC, Kwon YS, Kwon OJ. Use of silicone stents for the management of post-tuberculosis tracheobronchial stenosis. Eur Respir J. 2006; 28:1029–1035.4. Park HY, Kim H, Koh WJ, Suh GY, Chung MP, Kwon OJ. Natural stent in the management of post-intubation tracheal stenosis. Respirology. 2009; 14:583–588.5. Berraondo J, Novella L, Sanz F, Lluch R, de Casimiro E, Lloret T. Management of tracheobronchial amyloidosis with therapeutic bronchoscopic techniques. Arch Bronconeumol. 2013; 49:207–209.6. Alloubi I, Thumerel M, Begueret H, Baste JM, Velly JF, Jougon J. Outcomes after bronchoscopic procedures for primary tracheobronchial amyloidosis: retrospective study of 6 cases. Pulm Med. 2012; 2012:352719.7. Howard ME, Ireton J, Daniels F, Langton D, Manolitsas ND, Fogarty P, et al. Pulmonary presentations of amyloidosis. Respirology. 2001; 6:61–64.8. Fiorelli A, Accardo M, Galluccio G, Santini M. Tracheobronchial amyloidosis treated by endobronchial laser resection and self expanding Y stent. Arch Bronconeumol. 2013; 49:303–305.9. Stephens KE Jr, Wood DE. Bronchoscopic management of central airway obstruction. J Thorac Cardiovasc Surg. 2000; 119:289–296.10. Lund ME, Force S. Airway stenting for patients with benign airway disease and the Food and Drug Administration advisory: a call for restraint. Chest. 2007; 132:1107–1108.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effects of Placement of Bicanalicular Silicon Tube and Silicone Stent on Granuloma Formation in Endoscopic Intranasal Dacryocystorhinostomy
- The Effects of Placement of Silicone Tube and e-PTFE Stent in External Dacryocystorhinostomy
- A Case of Tracheal Stenosis Treated by Endotracheal Stent
- Prognostic Factors for Endotracheal Silicone Stenting in the Management of Inoperable Post-Intubation Tracheal Stenosis
- New expandable metallic stents: an experimental study in vessels of dogs
