A Case of IgG4-Related Disease Presenting as Massive Pleural Effusion and Thrombophlebitis
- Affiliations
-
- 1Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. minkyunghoon@korea.ac.kr
Abstract
- Immunoglobulin (Ig) G4-related disease is a recently recognized systemic fibroinflammatory condition characterized by a lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells with elevated circulating levels of IgG4. The disease can either be localized to one or two organs, or present as diffuse multi-organ disease. Furthermore, lesions in different organs can present simultaneously or metachronously. In the pulmonary manefestations, lesions associated with IgG4-related disease have been described in the lung parenchyma, airways and pleura, as well as the mediastinum. We report a case of IgG4-related disease presenting as massive pleural effusion and thrombophlebitis.
Keyword
MeSH Terms
Figure
-

Figure 1 (A-D) Imaging study on admission day showed thrombophlebitis of neck vein and enlarged lymph node in the left neck and axillar area with both pleural effusion and ascites and diffuse soft tissue edema. (A) Posterior-anterior (PA) view of chest X-ray. (B-D) Transverse section of chest computed tomography (CT). (E) Coronal section of chest CT. (F-H) Imaging study at 2 months after systemic steroid and anticoagulation showed markedly improved previous imaging finding. (F) PA view of chest X-ray. (G-I) Transverse section of chest CT. (J) Coronal section of chest CT.
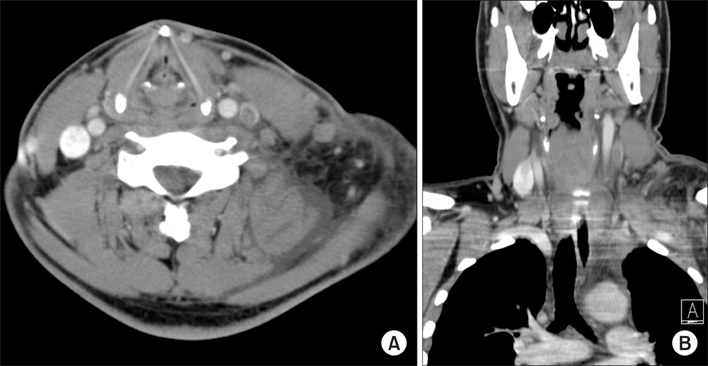
Figure 2 Neck computed tomography on admission day showed showed thrombophlebitis of neck vein and enlarged lymph node at left neck and axillar area. (A) Transverse section. (B) Coronal section.
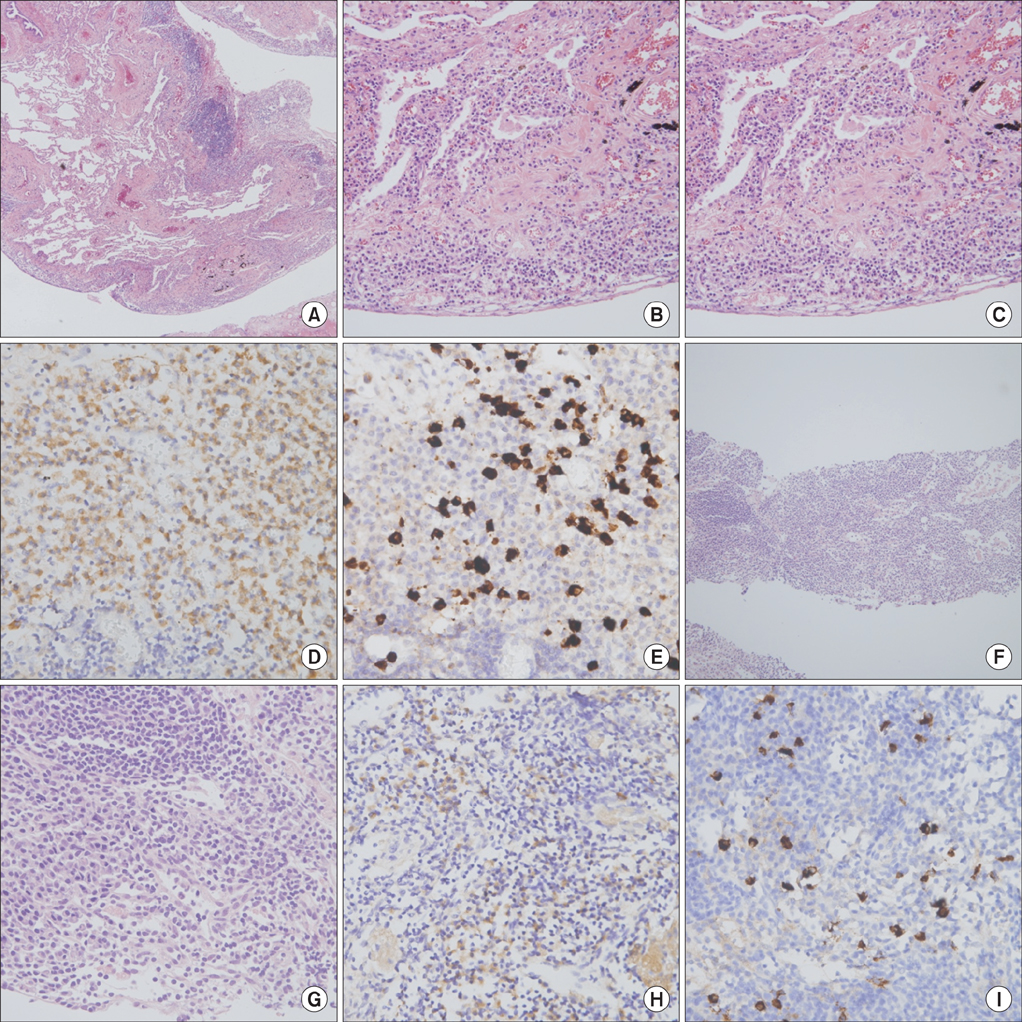
Figure 3 (A-E) Pleural biopsy showed chronic inflammation with lymphoplasmacytic infiltration and fibrosis (A, H&E stain, ×40; B, H&E stain, ×200; C, H&E stain, ×400; D, immunohistochemical stain for IgG, ×400; E, immunohistochemical stain for IgG4, ×400). (F-I) Lymph node biopsy of neck on previous admission also showed chronic inflammation with lymphoplasmacytic infiltration (F, H&E stain, ×40; G, H&E stain, ×400; H, immunohistochemical stain for IgG, ×400; I, immunohistochemical stain for IgG4, ×400).
Reference
-
1. Saeki T, Saito A, Hiura T, Yamazaki H, Emura I, Ueno M, et al. Lymphoplasmacytic infiltration of multiple organs with immunoreactivity for IgG4: IgG4-related systemic disease. Intern Med. 2006; 45:163–167.2. Ryu JH, Sekiguchi H, Yi ES. Pulmonary manifestations of immunoglobulin G4-related sclerosing disease. Eur Respir J. 2012; 39:180–186.3. Sarles H, Sarles JC, Muratore R, Guien C. Chronic inflammatory sclerosis of the pancreas-an autonomous pancreatic disease? Am J Dig Dis. 1961; 6:688–698.4. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738.5. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.6. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22:21–30.7. Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–1192.8. Masaki Y, Kurose N, Yamamoto M, Takahashi H, Saeki T, Azumi A, et al. Cutoff values of serum IgG4 and histopathological IgG4+ plasma cells for diagnosis of patients with IgG4-related disease. Int J Rheumatol. 2012; 2012:580814.9. Zen Y, Inoue D, Kitao A, Onodera M, Abo H, Miyayama S, et al. IgG4-related lung and pleural disease: a clinicopathologic study of 21 cases. Am J Surg Pathol. 2009; 33:1886–1893.10. Matsui S, Hebisawa A, Sakai F, Yamamoto H, Terasaki Y, Kurihara Y, et al. Immunoglobulin G4-related lung disease: clinicoradiological and pathological features. Respirology. 2013; 18:480–487.11. Kawakami N, Kawai K, Baba N, Ohshima K, Kanekura T. Immunoglobulin G4-positive multi-organ lymphoproliferative syndrome with antiphospholipid antibody syndrome. J Dermatol. 2012; 39:636–639.12. Tanigawa J, Daimon M, Murai M, Katsumata T, Tsuji M, Ishizaka N. Immunoglobulin G4-related coronary periarteritis in a patient presenting with myocardial ischemia. Hum Pathol. 2012; 43:1131–1134.13. Byeon K, Han J, Kim JS, Kim WS, Choe YH, Lee EJ, et al. Immunoglobulin G4-related periaortitis mimicking an intramural hematoma. Ann Thorac Surg. 2011; 92:1506–1508.14. Chari ST, Smyrk TC, Levy MJ, Topazian MD, Takahashi N, Zhang L, et al. Diagnosis of autoimmune pancreatitis: the Mayo Clinic experience. Clin Gastroenterol Hepatol. 2006; 4:1010–1016.15. Khosroshahi A, Carruthers MN, Deshpande V, Unizony S, Bloch DB, Stone JH. Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medicine (Baltimore). 2012; 91:57–66.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Extensive IgG4-Related Disease Presenting as Massive Pleural Effusion, Mediastinal Mass, and Mesenteric Lymphadenopathy in a 16-Year-Old Male
- A Case of Chronic Pancreatitis with Massive Pleural Effusion
- Refractory Pleural Effusion in Systemic Lupus Erythematosus Treated by Pleurectomy
- Non-IgG4-Related Fibrosclerosing Periaortitis with Multisystemic Involvement
- A Case of Ovarian Hyperstimulation Syndrome with Massive Pleural Effusion
