Tuberc Respir Dis.
2012 Jan;72(1):8-14.
Contributors of the Severity of Airflow Limitation in COPD Patients
- Hong Y
- Chae EJ
- Seo JB
- Lee JH
- Kim EK
- Lee YK
- Kim TH
- Kim WJ
- Lee JH

- Lee SM
- Lee S
- Lim SY
- Shin TR
- Yoon HI
- Sheen SS
- Ra SW
- Lee JS
- Huh JW
- Lee SD
- Oh YM
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine and Clinical Research Center for Chronic Obstructive Airway Diseases, Seoul, Korea. ymoh55@amc.seoul.kr
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Bundang CHA Hospital, CHA University College of Medicine, Seongnam, Korea.
- 4Department of Radiology, East-West Neo Medical Center, Kyunghee University School of Medicine, Seoul, Korea.
- 5Division of Pulmonology, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
- 6Department of Internal Medicine, College of Medicine, Kangwon National University, Chuncheon, Korea.
- 7Department of Internal Medicine, Ewha Womans University Mokdong Hospital, Ewha Womans University College of Medicine, Seoul, Korea.
- 8Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 9Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 10Division of Pulmonary and Critical Care Medicine, Department of Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 11Department of Internal Medicine, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
- 12Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 13Department of Pulmonary and Critical Care Medicine, Ajou University School of Medicine, Suwon, Korea.
- 14Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
Abstract
- BACKGROUND
Although airway obstruction in chronic obstructive pulmonary disease (COPD) is due to pathologic processes in both the airways and the lung parenchyma, the contribution of these processes, as well as other factors, have not yet been evaluated quantitatively. We therefore quantitatively evaluated the factors contributing to airflow limitation in patients with COPD.
METHODS
The 213 COPD patients were aged >45 years, had smoked >10 pack-years of cigarettes, and had a post-bronchodilator forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) <0.7. All patients were evaluated by medical interviews, physical examination, spirometry, bronchodilator reversibility tests, lung volume, and 6-minute walk tests. In addition, volumetric computed tomography (CT) was performed to evaluate airway wall thickness, emphysema severity, and mean lung density ratio at full expiration and inspiration. Multiple linear regression analysis was performed to identify the variables independently associated with FEV1 - the index of the severity of airflow limitation.
RESULTS
Multiple linear regression analysis showed that CT measurements of mean lung density ratio (standardized coefficient beta=-0.46; p<0.001), emphysema severity (volume fraction of the lung less than -950 HU at full inspiration; beta=-0.24; p<0.001), and airway wall thickness (mean wall area %; beta=-0.19, p=0.001), as well as current smoking status (beta=-0.14; p=0.009) were independent contributors to FEV1.
CONCLUSION
Mean lung density ratio, emphysema severity, and airway wall thickness evaluated by volumetric CT and smoking status could independently contribute to the severity of airflow limitation in patients with COPD.
Keyword
MeSH Terms
Figure
-
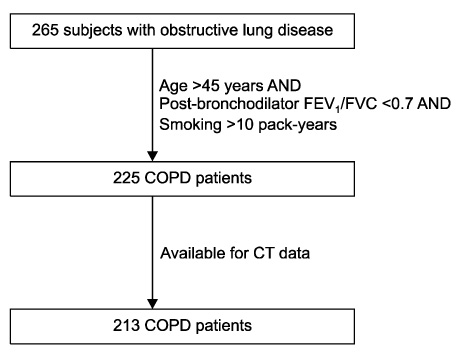
Figure 1 Selection of the study subjects from all subjects with obstructive lung disease. COPD: chronic obstructive pulmonary disease; CT: computed tomography.
Reference
-
1. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007. 176:532–555.2. Hogg JC. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet. 2004. 364:709–721.3. Celli BR. Roger S. Mitchell lecture. Chronic obstructive pulmonary disease phenotypes and their clinical relevance. Proc Am Thorac Soc. 2006. 3:461–465.4. Cerveri I, Dore R, Corsico A, Zoia MC, Pellegrino R, Brusasco V, et al. Assessment of emphysema in COPD: a functional and radiologic study. Chest. 2004. 125:1714–1718.5. Reilly J. Using computed tomographic scanning to advance understanding of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006. 3:450–455.6. Nakano Y, Wong JC, de Jong PA, Buzatu L, Nagao T, Coxson HO, et al. The prediction of small airway dimensions using computed tomography. Am J Respir Crit Care Med. 2005. 171:142–146.7. Hasegawa M, Nasuhara Y, Onodera Y, Makita H, Nagai K, Fuke S, et al. Airflow limitation and airway dimensions in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006. 173:1309–1315.8. Lee YK, Oh YM, Lee JH, Kim EK, Lee JH, Kim N, et al. Quantitative assessment of emphysema, air trapping, and airway thickening on computed tomography. Lung. 2008. 186:157–165.9. Kim WJ, Oh YM, Sung J, Kim TH, Huh JW, Jung H, et al. Lung function response to 12-week treatment with combined inhalation of long-acting beta2 agonist and glucocorticoid according to ADRB2 polymorphism in patients with chronic obstructive pulmonary disease. Lung. 2008. 186:381–386.10. Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005. 26:720–735.11. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.12. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005. 26:511–522.13. Wood SA, Zerhouni EA, Hoford JD, Hoffman EA, Mitzner W. Measurement of three-dimensional lung tree structures by using computed tomography. J Appl Physiol. 1995. 79:1687–1697.14. Nakano Y, Muro S, Sakai H, Hirai T, Chin K, Tsukino M, et al. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function. Am J Respir Crit Care Med. 2000. 162:1102–1108.15. Orlandi I, Moroni C, Camiciottoli G, Bartolucci M, Belli G, Villari N, et al. Spirometric-gated computed tomography quantitative evaluation of lung emphysema in chronic obstructive pulmonary disease: a comparison of 3 techniques. J Comput Assist Tomogr. 2004. 28:437–442.16. Washko GR, Criner GJ, Mohsenifar Z, Sciurba FC, Sharafkhaneh A, Make BJ, et al. Computed tomographic-based quantification of emphysema and correlation to pulmonary function and mechanics. COPD. 2008. 5:177–186.17. Bakhtavar K, Sedighi N, Moradi Z. Inspiratory and expiratory high-resolution computed tomography (HRCT) in patients with chemical warfare agents exposure. Inhal Toxicol. 2008. 20:507–511.18. Lucidarme O, Grenier PA, Cadi M, Mourey-Gerosa I, Benali K, Cluzel P. Evaluation of air trapping at CT: comparison of continuous-versus suspended-expiration CT techniques. Radiology. 2000. 216:768–772.19. Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004. 350:2645–2653.20. Gevenois PA, De Vuyst P, Sy M, Scillia P, Chaminade L, de Maertelaer V, et al. Pulmonary emphysema: quantitative CT during expiration. Radiology. 1996. 199:825–829.21. Omori H, Nakashima R, Otsuka N, Mishima Y, Tomiguchi S, Narimatsu A, et al. Emphysema detected by lung cancer screening with low-dose spiral CT: prevalence, and correlation with smoking habits and pulmonary function in Japanese male subjects. Respirology. 2006. 11:205–210.22. Orlandi I, Moroni C, Camiciottoli G, Bartolucci M, Pistolesi M, Villari N, et al. Chronic obstructive pulmonary disease: thin-section CT measurement of airway wall thickness and lung attenuation. Radiology. 2005. 234:604–610.23. Berger P, Perot V, Desbarats P, Tunon-de-Lara JM, Marthan R, Laurent F. Airway wall thickness in cigarette smokers: quantitative thin-section CT assessment. Radiology. 2005. 235:1055–1064.24. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Golobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO workshop report. 2009. [place unknown]: GOLD.25. Dransfield MT, Washko GR, Foreman MG, Estepar RS, Reilly J, Bailey WC. Gender differences in the severity of CT emphysema in COPD. Chest. 2007. 132:464–470.26. Martinez FJ, Curtis JL, Sciurba F, Mumford J, Giardino ND, Weinmann G, et al. Sex differences in severe pulmonary emphysema. Am J Respir Crit Care Med. 2007. 176:243–252.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pathophysiology of Chronic Obstructive Pulmonary Disease
- Pathophysiology of Chronic Obstructive Pulmonary Disease
- Association between Albuminuria and Severity of Chronic Obstructive Pulmonary Disease: The 8th Korea National Health and Nutrition Examination Survey (2019)
- Prevalence of Combined Bronchial Asthma with COPD in Patients with Moderate to Severe Air flow Limitation
- The Importance of Early Chronic Obstructive Pulmonary Disease: A Lecture from 2022 Asian Pacific Society of Respirology
