Infection Rate of Chlamydia pneumoniae in Patients with Chronic Cough
- Affiliations
-
- 1Department of Internal Medicine, Hallym University College of Medicine, Chuncheon, Korea. bfspark@medimail.co.kr
Abstract
- BACKGROUND
Persistent cough has recently been found to be associated with Chlamydia pneumoniae infection. We aimed to investigate the infection rate of C. pneumonia in adult patients with chronic cough.
METHODS
We recruited 68 patients with persistent cough lasting in excess of 3 weeks, who visited Kangdong Sacred Heart Hospital from January 2005 to August 2005. On the first visit, chest and paranasal sinuses radiography, skin prick test of common allergens, and induced sputum samples for C. pneumoniae were performed in all of patients. Further evaluation for diagnosis included a methacholine provocation test and eosinophil counts in induced sputum.
RESULTS
The most common cause of chronic cough was upper airway cough syndrome (UACS) (26.5%), followed by eosinophilic bronchitis (20.6%) and cough variant asthma (16.2%). Idiopathic chronic cough was the cause in 33.8% of patients. The mean duration of cough was 11.7 months. C. pneumoniae was isolated by polymerase chain reaction (PCR) from one patient who had upper respiratory air way syndrome.
CONCLUSION
Chlamydia pneumoniae appears to have a minor role as a cause of chronic cough in patients.
MeSH Terms
Figure
-
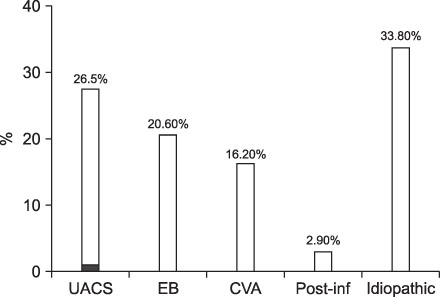
Figure 1 Causes of chronic cough in patients coming to a clinic. This group of 68 patients had UACS, EB, CVA, Pos-inf and idiopathic chronic cough. Chlamydia pneumoniae DNA was detected in one patient (dark gray). UACS: upper airway cough syndrome; EB: eosinophillic bronchitis; CVA: cough variant asthma; Post-inf: post-infectious.
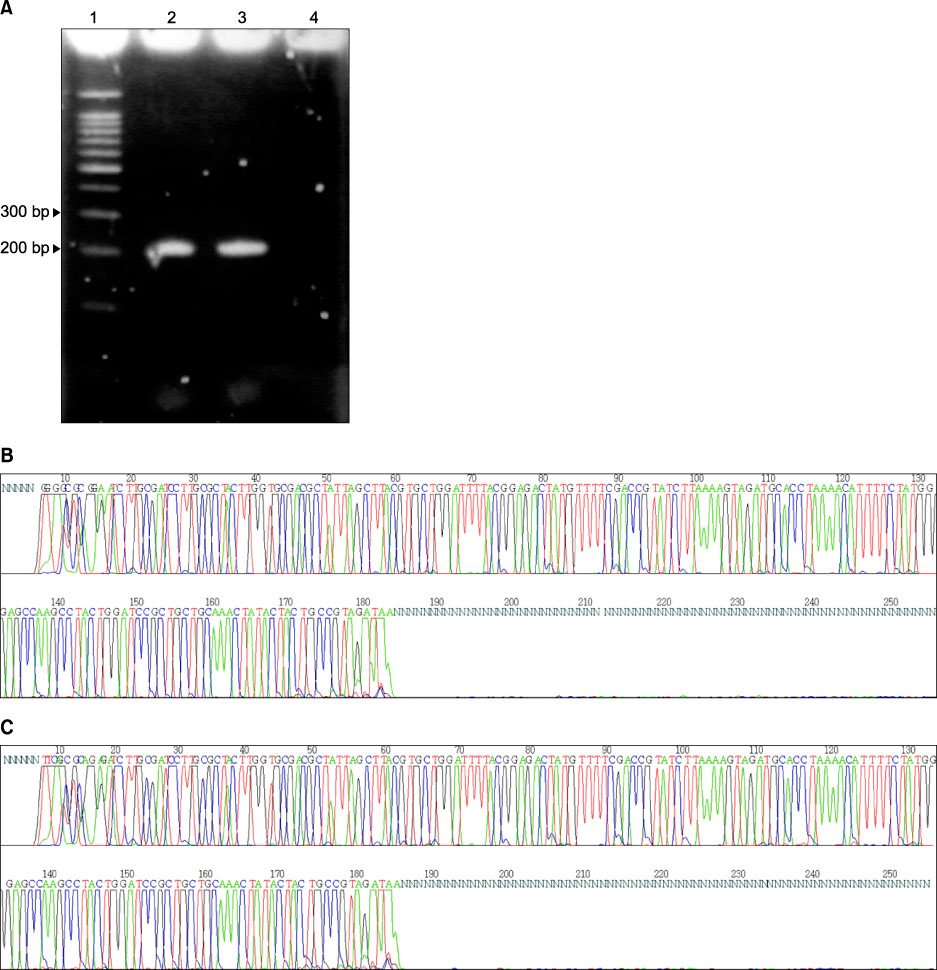
Figure 2 Agarose gel images of the amplification of C. pneumoniae DNA from patient sample (A). Samples were amplified by nested PCR using CP-1, CP-2 primer set and then CPC, CPD primer set. Lane 1: molecular size standards; lane 2: positive control; lane 3: positive sample from patient (207 bp); Lane 4: negative control. DNA sequencing results from the PCR product of the patient (B) and positive control (C) confirmed PCR product was cDNA of C. pneumoniae.
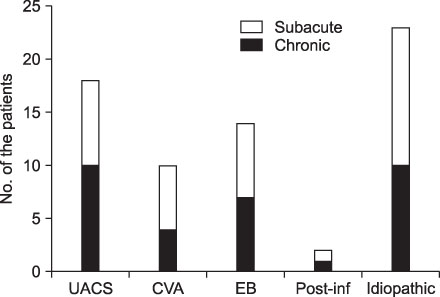
Figure 3 Frequency of cases classified as subacute and chronic cough. The differences were not significant (p>0.05). UACS: upper airway cough syndrome; EB: eosinophillic bronchitis; CVA: cough variant asthma; Post-inf: post-infectious cough.
Reference
-
1. Irwin RS, Rosen MJ, Braman SS. Cough. A comprehensive review. Arch Intern Med. 1977. 137:1186–1191.2. Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981. 123:413–417.3. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990. 141:640–647.4. Brightling CE, Ward R, Goh KL, Wardlaw AJ, Pavord ID. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med. 1999. 160:406–410.5. Grayston JT, Wang S. New knowledge of chlamydiae and the diseases they cause. J Infect Dis. 1975. 132:87–105.6. Kuo CC, Jackson LA, Campbell LA, Grayston JT. Chlamydia pneumoniae (TWAR). Clin Microbiol Rev. 1995. 8:451–461.7. Hyman CL, Augenbraun MH, Roblin PM, Schachter J, Hammerschlag MR. Asymptomatic respiratory tract infection with Chlamydia pneumoniae TWAR. J Clin Microbiol. 1991. 29:2082–2083.8. Hyman CL, Roblin PM, Gaydos CA, Quinn TC, Schachter J, Hammerschlag MR. Prevalence of asymptomatic nasopharyngeal carriage of Chlamydia pneumoniae in subjectively healthy adults: assessment by polymerase chain reaction-enzyme immunoassay and culture. Clin Infect Dis. 1995. 20:1174–1178.9. Miyashita N, Fukano H, Yoshida K, Niki Y, Matsushima T. Chlamydia pneumoniae infection in adult patients with persistent cough. J Med Microbiol. 2003. 52:265–269.10. Kim WJ, Lee HY, Lee ME, Lee SJ. Serology of Chlamydia pneumoniae in patients with chronic cough. Respirology. 2006. 11:805–808.11. Smieja M, Mahony JB, Goldsmith CH, Chong S, Petrich A, Chernesky M. Replicate PCR testing and probit analysis for detection and quantitation of Chlamydia pneumoniae in clinical specimens. J Clin Microbiol. 2001. 39:1796–1801.12. Lee HS, Chun BY, Jin SH, Lee WK. Infection rate of Chlamydia pneumoniae by serological antibody test between patients with respiratory symptoms and control group. Korean J Clin Microbiol. 2004. 7:31–37.13. Gnarpe J, Eriksson K. Sample preparation for Chlamydia pneumoniae PCR. APMIS. 1995. 103:307–308.14. Tong CY, Sillis M. Detection of Chlamydia pneumoniae and Chlamydia psittaci in sputum samples by PCR. J Clin Pathol. 1993. 46:313–317.15. Lee WK. Chlamydia pneumoniae and Atherosclerosis. Korean J Clin Microbiol. 2001. 4:78–81.16. Lee EM, Oh DJ, Hwang GS, Ahn JC, Song WH, Lim DS, et al. Chronic chlamydia pneumoniae infection as a risk factor for acute myocardial infarction in Korea. Korean Circ J. 2000. 30:407–415.17. File TM Jr, Tan JS, Plouffe JF. The role of atypical pathogens: Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumophila in respiratory infection. Infect Dis Clin North Am. 1998. 12:569–592.18. Hahn DL, Anttila T, Saikku P. Association of Chlamydia pneumoniae IgA antibodies with recently symptomatic asthma. Epidemiol Infect. 1996. 117:513–517.19. Black PN, Scicchitano R, Jenkins CR, Blasi F, Allegra L, Wlodarczyk J, et al. Serological evidence of infection with Chlamydia pneumoniae is related to the severity of asthma. Eur Respir J. 2000. 15:254–259.20. Miyashita N, Kubota Y, Nakajima M, Niki Y, Kawane H, Matsushima T. Chlamydia pneumoniae and exacerbations of asthma in adults. Ann Allergy Asthma Immunol. 1998. 80:405–409.21. Black PN, Blasi F, Jenkins CR, Scicchitano R, Mills GD, Rubinfeld AR, et al. Trial of roxithromycin in subjects with asthma and serological evidence of infection with Chlamydia pneumoniae. Am J Respir Crit Care Med. 2001. 164:536–541.22. Ferrari M, Poli A, Olivieri M, Verlato G, Tardivo S, Nicolis M, et al. Respiratory symptoms, asthma, atopy and Chlamydia pneumoniae IgG antibodies in a general population sample of young adults. Infection. 2002. 30:203–207.23. Dowell SF, Peeling RW, Boman J, Carlone GM, Fields BS, Guarner J, et al. Standardizing Chlamydia pneumoniae assays: recommendations from the Centers for Disease Control and Prevention (USA) and the Laboratory Centre for Disease Control (Canada). Clin Infect Dis. 2001. 33:492–503.24. Hermann C, Gueinzius K, Oehme A, Von Aulock S, Straube E, Hartung T. Comparison of quantitative and semiquantitative enzyme-linked immunosorbent assays for immunoglobulin G against Chlamydophila pneumoniae to a microimmunofluorescence test for use with patients with respiratory tract infections. J Clin Microbiol. 2004. 42:2476–2479.25. Park J, Kim JK, Rheem I, Kim J. Evaluation of Seeplex Pneumobacter multiplex PCR kit for the detection of respiratory bacterial pathogens in pediatric patients. Korean J Lab Med. 2009. 29:307–313.26. Park SE, Choi SE, Jung HS, Kwak YH, Lee HJ. Detection of Chlamydia pneumoniae by use of the nested polymerase chain reaction in children with lower respiratory tract infection. Korean J Infect Dis. 1999. 31:197–202.27. Birkebaek NH, Jensen JS, Seefeldt T, Degn J, Huniche B, Andersen PL, et al. Chlamydia pneumoniae infection in adults with chronic cough compared with healthy blood donors. Eur Respir J. 2000. 16:108–111.28. Boman J, Gaydos CA, Quinn TC. Molecular diagnosis of Chlamydia pneumoniae infection. J Clin Microbiol. 1999. 37:3791–3799.29. Block S, Hedrick J, Hammerschlag MR, Cassell GH, Craft JC. Mycoplasma pneumoniae and Chlamydia pneumoniae in pediatric community-acquired pneumonia: comparative efficacy and safety of clarithromycin vs. erythromycin ethylsuccinate. Pediatr Infect Dis J. 1995. 14:471–477.30. Hammerschlag MR, Chirgwin K, Roblin PM, Gelling M, Dumornay W, Mandel L, et al. Persistent infection with Chlamydia pneumoniae following acute respiratory illness. Clin Infect Dis. 1992. 14:178–182.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Chlamydia Antibody Using Micro-immunofluorescence in Acute Myocardiac Infarction
- Enzyme-linked Immunosorbent Assays for Antibodies against Chlamydia Pneumoniae Compared with Microimmunofluorescence Test with Patients with Chronic Cough
- Detection of Chlamydia pneumoniae by 'Touchdown' PCR
- Detection of Chlamydia pneumoniae by Use of the Nested Polymerase Chain Reaction in Children with Lower Respiratory Tract Infection
- Meaning of serum antibody to Chlamydia pneumoniae in patients with restenosis after coronary balloon angioplasty or stent insertion
