Tuberc Respir Dis.
2010 Jul;69(1):43-47.
Non-tuberculous Mycobacterial Lung Disease Presenting as a Solitary Pulmonary Nodule
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. jwmoon@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3The Institute of Chest Diseases, Yonsei University College of Medicine, Seoul, Korea.
Abstract
- We report a case of Mycobacterium intracellulare pulmonary infection presenting as a solitary pulmonary nodule (SPN). A 35-year-old male was admitted due to a SPN in the right upper lobe which was detected on the chest radiography being examed due to recurrent cough for 1 year. The computed tomography (CT) revealed a spiculated nodule containing air-bronchogram, which was suspicious of malignancy. We performed transbronchial biopsy and the pathology showed granulomatous inflammation with caseous necrosis. Under the presumptive diagnosis of pulmonary tuberculosis, we started anti-tuberculous medication including isoniazid, rifampin, ethambutol, and pyrazinamide. In one month, however, the sputum culture was positive for Mycobacterium intracellulare. The follow-up chest CT showed slight aggravation of the previous lesions. Under the final diagnosis of Mycobacterium intracellulare pulmonary infection presenting as a solitary pulmonary nodule, we changed the regimen to rifampin, ethambutol, and clarithromycin. The follow-up chest CT after the completion of treatment, revealed resolution of the previous lesions.
MeSH Terms
-
Adult
Biopsy
Clarithromycin
Cough
Ethambutol
Follow-Up Studies
Humans
Inflammation
Isoniazid
Lung
Lung Diseases
Male
Mycobacterium avium Complex
Mycobacterium Infections, Nontuberculous
Necrosis
Pyrazinamide
Rifampin
Solitary Pulmonary Nodule
Sputum
Thorax
Tuberculosis
Tuberculosis, Pulmonary
Clarithromycin
Ethambutol
Isoniazid
Pyrazinamide
Rifampin
Figure
-

Figure 1 The initial chest X-ray shows a nodular opacity in the right upper lung field.

Figure 2 The initial chest CT shows a spiculated nodule with airbronchogram in the right upper lobe.

Figure 3 The histologic finding of the transbronchial biopsy specimen shows chronic granulomatous inflammation with caseous necrosis (H&E stain, ×100).
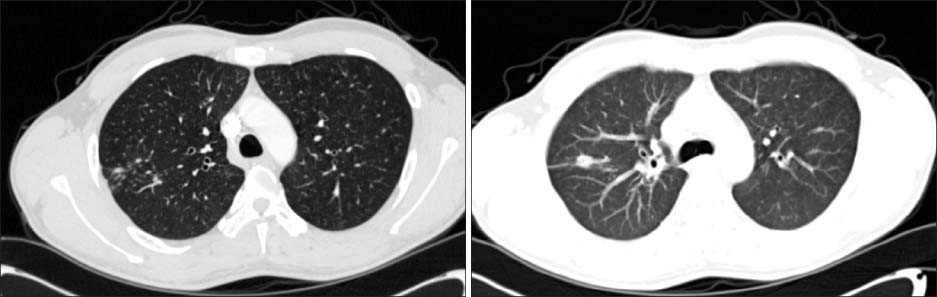
Figure 4 The chest CT reveals multiple newly-developed centrilobular nodules after the completion of six-month anti-tuberculous chemotherapy.

Figure 5 The follow-up chest CT after the completion of anti-Mycobacterium intracellulare chemotherapy shows the resolution of previous nodular lesions.
Reference
-
1. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007. 175:367–416.2. Koh WJ, Kwon OJ, Lee KS. Diagnosis and treatment of nontuberculous mycobacterial pulmonary diseases: a Korean perspective. J Korean Med Sci. 2005. 20:913–925.3. Albelda SM, Kern JA, Marinelli DL, Miller WT. Expanding spectrum of pulmonary disease caused by nontuberculous mycobacteria. Radiology. 1985. 157:289–296.4. Lillington GA, Caskey CI. Evaluation and management of solitary and multiple pulmonary nodules. Clin Chest Med. 1993. 14:111–119.5. Yi CA, Lee KS, Kim EA, Han J, Kim H, Kwon OJ, et al. Solitary pulmonary nodules: dynamic enhanced multi-detector row CT study and comparison with vascular endothelial growth factor and microvessel density. Radiology. 2004. 233:191–199.6. Lee HS, Oh JY, Lee JH, Yoo CG, Lee CT, Kim YW, et al. Response of pulmonary tuberculomas to anti-tuberculous treatment. Eur Respir J. 2004. 23:452–455.7. Tanaka E, Amitani R, Kuze F. Clinical features of the patients with "secondary infection" of Mycobacterium avium complex: radiographic pattern of progressions in the patients with and without underlying pulmonary conditions. Kekkaku. 1993. 68:57–61.8. Lynch DA, Simone PM, Fox MA, Bucher BL, Heinig MJ. CT features of pulmonary Mycobacterium avium complex infection. J Comput Assist Tomogr. 1995. 19:353–360.9. Gribetz AR, Damsker B, Bottone EJ, Kirschner PA, Teirstein AS. Solitary pulmonary nodules due to nontuberculous mycobacterial infection. Am J Med. 1981. 70:39–43.10. Kobashi Y, Yoshida K, Miyashita N, Niki Y, Matsushima T. Pulmonary Mycobacterium avium disease with a solitary pulmonary nodule requiring differentiation from recurrence of pulmonary adenocarcinoma. Intern Med. 2004. 43:855–860.11. Hahm CR, Park HY, Jeon K, Um SW, Suh GY, Chung MP, et al. Solitary pulmonary nodules caused by Mycobacterium tuberculosis and Mycobacterium avium complex. Lung. 2010. 188:25–31.12. Kwon YS, Koh WJ, Kwon OJ, Lee NY, Han J, Lee KS, et al. Mycobacterium abscessus pulmonary infection presenting as a solitary pulmonary nodule. Intern Med. 2006. 45:169–171.13. Ra SW, Lee KH, Jung JY, Kang HS, Park IN, Choi HS, et al. Mycobacterium Kansasii disease presenting as a lung mass and bronchial anthracofibrosis. Tuberc Respir Dis. 2006. 60:464–468.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of the Solitary Pulmonary Nodule Diagnosed as Pulmonary Paragonimiasis
- Bronchioloalveolar Cell Carcinoma in Solitary Pulmonary Nodule(SPN) with Cavitary Lesion
- Primary Intrapulmonary Thymoma Presenting as a Solitary Pulmonary Nodule
- A Case of Tuberculous Pleural Effusion Developed after Percutaneous Needle Biopsy of a Solitary Pulmonary Nodule
- Thoracoscopic Needle Aspiration Biopsy for a Centrally Located Solitary Pulmonary Nodule
