Tuberc Respir Dis.
2009 Jun;66(6):444-450.
The Role and Significance of Biomarker for Plasma G-CSF in Patients with Primary Lung Cancer
- Affiliations
-
- 1Department of Internal Medicine, Wonkwang University College of Medicine, Iksan, Korea. yshpul@wonkwang.ac.kr
- 2Department of Pathology, Wonkwang University College of Medicine, Iksan, Korea.
- 3Department of Therapeutic Radiology & Oncology, Wonkwang University College of Medicine, Iksan, Korea.
- 4Department of Radiology, Wonkwang University College of Medicine, Iksan, Korea.
- 5Department of Clinical Pathology, Wonkwang University College of Medicine, Iksan, Korea.
- 6Good Cell Life, Inc., Seoul, Korea.
- 7Department of Thoracic Surgery, Wonkwang University College of Medicine, Iksan, Korea.
Abstract
-
BACKGROUND: Biomarkers for cancer have several potential clinical uses, including the following: early cancer detection, monitoring for recurrence prognostication, and risk stratification. However, no biomarker has been shown to have adequate sensitivity and specificity. Many investigators have tried to validate biomarkers for the early detection and recurrence of lung cancer. To evaluate plasma G-CSF as such a biomarker, protein levels were measured and were found to correlate with the clinicopathological features of primary lung tumors.
METHODS
Between December 2006 and May 2008, 100 patients with histologically-validated primary lung cancer were enrolled into this study. To serve as controls, 127 healthy volunteers were enrolled into this study. Plasma G-CSF levels were measured in lung cancer patients using the sandwich ELISA system (R & D inc.) prior to treatment.
RESULTS
The mean plasma G-CSF levels were 12.2+/-0.3 pg/mL and 46.0+/-3.8 pg/mL (mean+/-SE) in the normal and in the cancer groups, respectively. In addition, plasma G-CSF levels were higher in patients with early lung cancer than in healthy volunteers (p<.001). Plasma G-CSF levels were higher in patients who were under 65 years old or smokers. Within the cancer group, plasma G-CSF levels were higher in patients with non small cell lung cancer than in patients with small cell lung cancer (p<.05). Overall, plasma G-CSF levels were shown to increase dependent upon the type of lung cancer diagnsosed. In the order from highest to lowest, the levels of plasma G-CSF tended to decrease in the following order: large cell carcinoma, squamous cell carcinoma, adenocarcinoma, and bronchioloalveolar carcinoma. Plasma G-CSF levels tended to be higher in patients with advanced TNM stage than in localized TNM stage (I, II
Plasma G-CSF level were significantly increased in patients with lung cancer, and in especially advanced TNM stage. These results suggest that plasma G-CSF can be used to support the diagnostic process of lung cancer staging and as an indicator of metastasis.
MeSH Terms
-
Adenocarcinoma
Adenocarcinoma, Bronchiolo-Alveolar
Adrenal Glands
Biomarkers
Carcinoma, Large Cell
Carcinoma, Squamous Cell
Enzyme-Linked Immunosorbent Assay
Granulocyte Colony-Stimulating Factor
Humans
Lung
Lung Neoplasms
Neoplasm Metastasis
Plasma
Recurrence
Research Personnel
Small Cell Lung Carcinoma
Granulocyte Colony-Stimulating Factor
Figure
-
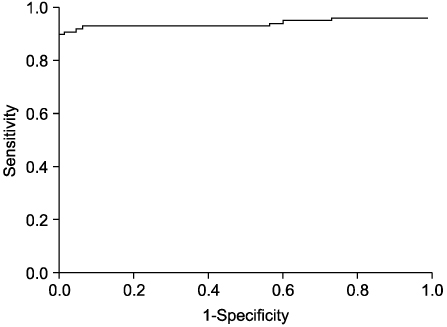
Figure 1 Receiver operator characteristic (ROC) curve for plasma G-CSF concentration. There were ROC curve for plasma G-CSF of lung cancer and normal person. When plasma G-CSF's cut-off value was 21 pg/mL, we determinated sensitivity was 90%, and specificity was 99%.
Reference
-
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005. 55:74–108.2. Mountain CF. A new international staging system for lung cancer. Chest. 1986. 89:225S–233S.3. Albain KS, Crowley JJ, Livingston RB. Long-term survival and toxicity in small cell lung cancer. Expanded Southwest Oncology Group experience. Chest. 1991. 99:1425–1432.4. Cooper DL. Goldman L, Bennett JC. Tumor markers. Cecil textbook of medicine. 2000. 21st ed. Philadelphia: W.B. Saunders company;1039–1042.5. Müller LC, Gasser R, Huber H, Klingler A, Salzer GM. Neuron-specific enolase (NSE) in small-cell lung cancer: longitudinal tumors marker evaluation. Lung Cancer. 1992. 8:29–36.6. Akoun GM, Scarna HM, Milleron BJ, Bénichou MP, Herman DP. Serum neuron-specific enolase: a marker for disease extent and response to therapy for small-cell lung cancer. Chest. 1985. 87:39–43.7. Bonomi P, Gale M, Rowland K, Taylor SG 4th, Purl S, Reddy S, et al. Pre-treatment prognostic factors in stage III non-small cell lung cancer patients receiving combined modality treatment. Int J Radiat Oncol Biol Phys. 1991. 20:247–252.8. Karnak D, Ulubay G, Kayacan O, Beder S, Ibis E, Oflaz G. Evaluation of Cyfra 21-1: a potential tumor marker for non-small cell lung carcinomas. Lung. 2001. 179:57–65.9. McDermott RS, Deneux L, Mosseri V, Védrenne J, Clough K, Fourquet A, et al. Circulating macrophage colony stimulating factor as a marker of tumor progression. Eur Cytokine Netw. 2002. 13:121–127.10. Miyagawa K, Chiba S, Shibuya K, Piao YF, Matsuki S, Yokota J, et al. Frequent expression of receptors for granulocyte-macrophage colony-stimulating factor on human nonhematopoietic tumor cell lines. J Cell Physiol. 1990. 143:483–487.11. Turner AM, Zsebo KM, Martin F, Jacobsen FW, Bennett LG, Broudy VC. Nonhematopoietic tumor cell lines express stem cell factor and display c-kit receptors. Blood. 1992. 80:374–381.12. Tani K, Ozawa K, Ogura H, Shimane M, Shirafuji N, Tsuruta T, et al. Expression of granulocyte and granulocyte macrophage colony-stimulating factors by human non-hematopoietic tumor cells. Growth Factors. 1990. 3:325–331.13. Yee LD, Liu L. The constitutive production of colony stimulating factor 1 by invasive human breast cancer cells. Anticancer Res. 2000. 20:4379–4383.14. Mroczko B, Groblewska M, Wereszczyńska-Siemiatkowska U, Okulczyk B, Kedra B, Laszewicz W, et al. Serum macrophage-colony stimulating factor levels in colorectal cancer patients correlate with lymph node metastasis and poor prognosis. Clin Chim Acta. 2007. 380:208–212.15. Usami N, Uchiyama M, Kawaguchi K, Yasuda A, Ito S, Yokoi K. Granulocyte colony-stimulating factor-producing malignant pleural mesothelioma. J Thorac Oncol. 2007. 2:257–258.16. Kobashi Y, Okimoto N, sakamoto K. Squamous cell carcinoma of the lung producing granulocyte colonystimulating factor and resembling a malignant pleural mesothelioma. Intern Med. 2004. 43:111–116.17. Buccheri G, Ferrigno D. Lung tumor markers of cytokeratin origin: an overview. Lung Cancer. 2001. 34:Suppl 2. S65–S69.18. Body JJ, Sculier JP, Raymakers N, Paesmans M, Ravez P, Libert P, et al. Evaluation of squamous cell carcinoma antigen as a new marker for lung cancer. Cancer. 1990. 65:1552–1556.19. Buccheri G, Ferrigno D. Usefulness of tissue polypeptide antigen in staging, monitoring, and prognosis of lung cancer. Chest. 1988. 93:565–570.20. Sculier JP, Body JJ, Jacobowitz D, Fruhling J. Value of CEA determination in biological fluids and tissues. Eur J Cancer Clin Oncol. 1987. 23:1091–1093.21. Mino N, Iio A, Hamamoto K. Availability of tumor-antigen 4 as a marker of squamous cell carcinoma of the lung and other organs. Cancer. 1988. 62:730–734.22. Wieskopf B, Demangeat C, Purohit A, Stenger R, Gries P, Kreisman H, et al. Cyfra 21-1 as a biologic marker of non-small cell lung cancer: evaluation of sensitivity, specificity, and prognostic role. Chest. 1995. 108:163–169.23. Mroczko B, Szmitkowski M, Okulczyk B. Granulocyte-colony stimulating factor (G-CSF) and macrophage-colony stimulating factor (M-CSF) in colorectal cancer patients. Clin Chem Lab Med. 2002. 40:351–355.24. Mroczko B, Szmitkowski M. Hematopoietic cytokines as tumor markers. Clin Chem Lab Med. 2004. 42:1347–1354.25. Asano S, Urabe A, Okabe T, Sato N, Kondo Y. Demonstration of granulopoietic factor(s) in the plasma of nude mice transplanted with a human lung cancer and in the tumor tissue. Blood. 1977. 49:845–852.26. Watari K, Asano S, Shirafuji N, Kodo H, Ozawa K, Takaku F, et al. Serum granulocyte colony-stimulating factor levels in healthy volunteers and patients with various disorders as estimated by enzyme immunoassay. Blood. 1989. 73:117–122.27. Hasegawa S, Suda T, Negi K, Hattori Y. Lung large cell carcinoma producing granulocyte-colony stimulating factor. Ann Thorac Surg. 2007. 83:308–310.28. Tsuruta N, Yatsunami J, Takayama K, Nakanishi Y, Ichinose Y, Hara N. Granulocyte-macrophage-colony stimulating factor stimulates tumor invasiveness in squamous cell lung carcinoma. Cancer. 1998. 82:2173–2183.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomarkers for Lung Cancer
- Surgical Treatment for Multiple Primary Lung Cancer: Report of 2 cases
- Comparison of Clinical Feature, CSF Cytology, Neuroimaging, and CSF Biochemical Marker in Leptomeningeal Metastasis
- Changes of Gas Values in the CSF and Blood during Sustained Hypoventilation
- Biomarker testing of cytology specimens in personalized medicine for lung cancer patients
