Mediastinal Bronchogenic Cyst, which was Grown Rapidly
- Affiliations
-
- 1Department of Internal medicine, Soonchunhyang University College of Medicine, Seoul, Korea. kukim@hosp.sch.ac.kr
- 2Department of Chest Surgery, Soonchunhyang University College of Medicine, Seoul, Korea.
- 3Department of Radiology, Soonchunhyang University College of Medicine, Seoul, Korea.
- 4Department of Pathology, Soonchunhyang University College of Medicine, Seoul, Korea.
Abstract
- Bronchogenic cyst arises from anomalous budding of the primitive foregut during embryonic development and it represents a part of the spectrum of bronchopulmonary foregut malformations. Approximately two-thirds of the malformations are found within the mediastinum, and one-third are found in the lung parenchyma. The prevalence of bronchogenic cyst is unknown, presumably because most patients are asymptomatic. Incidentally detected bronchogenic cysts are usually removed at the time of diagnosis. We do not know how and why bronchogenic cysts grow. We recently experienced a case of rapidly growing mediastinal mass in a young adult, and this presented as a huge mass that had newly developed within one year. This mass was pathologically confirmed to be a bronchogenic cyst. We report on this case of a rapidly growing bronchogenic cyst, which is a rare characteristic of this type of cyst.
Keyword
MeSH Terms
Figure
-
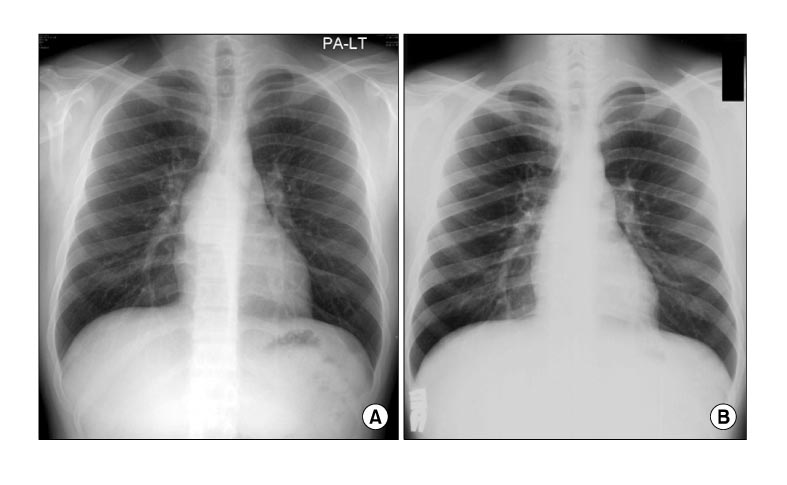
Figure 1 Chest PA finding of 20 year old male at first visit and 1 year ago, well defined mass like opacity was showed at subcarinal area which was almost fist size of child (A). However 1 year ago, the mass was not detected (B).

Figure 2 Chest computed tomography of the presented male. There was about 5.6×4.8×7 cm sized, well defined, cystic mass at right subcarinal area. Bronchus intermedius of right lung was compressed by the cystic mass.

Figure 3 Bronchoscopic finding of right bronchus intermedius, posterior wall of the bronchus was bulged by extrinsic compression, but mucosal wall looked intact.
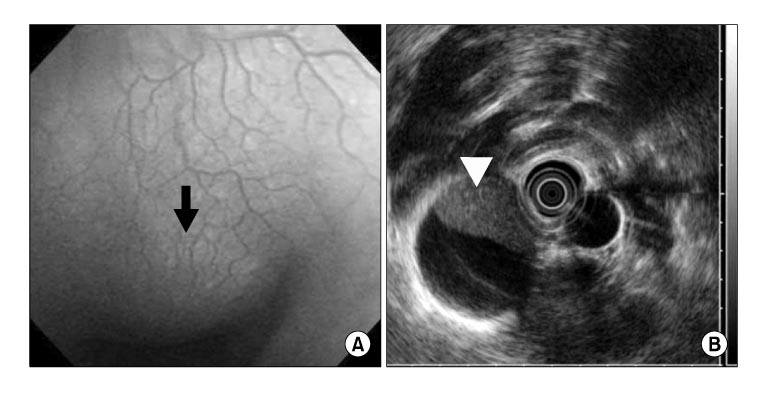
Figure 4 Gastroscopy (A) and endoscopic ultrasound (B) findings of the presented male, there was an indentation of esophagus at 25~32 cm from incisor (arrow). Endoscopic ultrasound showed about 6.6 cm sized hypoechoic cyst. Echogenic material of the inside of cyst was changed their location by position (arrow head).
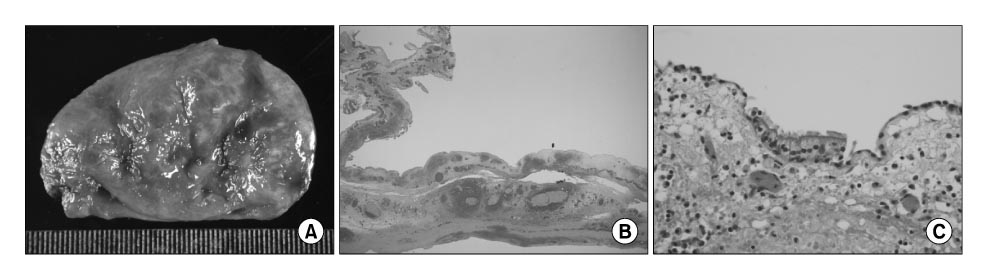
Figure 5 Gross and microscopic findings after surgical excision from the presented male. A brown red colored unilocular cyst was measured 6×4×1 cm. Wall of the cyst looked grossly smooth and spherical fibrotic tissue which was accompanied multiple and focal hemorrhage (A). Microscopic finding demonstrated a cyst wall which had contained airway components such as cartilage plate and smooth muscle (B, ×40). Magnified photograph showed single layer of ciliated columnar epithelium as like bronchial epithelium with goblet cells (C, H&E stain, ×200).
Reference
-
1. Kirwan WO, Walbaum PR, McCormack RJ. Cystic intrathoracic derivatives of the foregut and their complications. Thorax. 1973. 28:424–428.2. Haller JA Jr, Golladay ES, Pickard LR, Tepas JJ 3rd, Shorter NA, Shermeta DW. Surgical management of lung bud anomalies: lobar emphysema, bronchogenic cyst, cystic adenomatoid malformation, and intralobar pulmonary sequestration. Ann Thorac Surg. 1979. 28:33–43.3. Maier HC. Bronchiogenic cysts of the mediastinum. Ann Surg. 1948. 127:476–502.4. You M, Park S. Congenital bronchogenic cyst: report of a case. J Korean Surg Soc. 1967. 9:537–540.5. Kim KH, Kwon SS, Yoon SJ, Kim YK, Han KD, Moon HS, et al. A case of congenital bronchogenic cyst with infection. Tuberc Respir Dis. 1990. 37:323–328.6. Kim YW, Lee SH, Hong SC, Lee HH, Park SJ, Lee GJ, et al. A case report of a bronchogenic cyst misconceived to lung cancer. Tuberc Respir Dis. 2003. 55:526–530.7. Kim GH, Kim KH, Kim MS, Park JE, Kim DJ, Son HS, et al. A case of pulmonary aspergilloma in bronchogenic cyst associated with an actinomycosis. Tuberc Respir Dis. 2004. 57:584–588.8. Choi KA, Koh WJ, Lee KS, Han J, Kim K. Multicystic pulmonary parenchymal lesions in a young adult with hemoptysis. Tuberc Respir Dis. 2007. 62:71–73.9. Sarper A, Ayten A, Golbasi I, Demircan A, Isin E. Bronchogenic cyst. Tex Heart Inst J. 2003. 30:105–108.10. McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, Matsumoto S. Bronchogenic cyst: imaging features with clinical and histopathologic correlation. Radiology. 2000. 217:441–446.11. Kramer H, van Putten JW, Douma WR, Smidt AA, van Dullemen HM, Groen HJ. Technical description of endoscopic ultrasonography with fine-needle aspiration for the staging of lung cancer. Respir Med. 2005. 99:179–185.12. Kawase Y, Takahashi M, Takemura H, Tomita S, Watanabe G. Surgical treatment of a bronchogenic cyst in the interatrial septum. Ann Thorac Surg. 2002. 74:1695–1697.13. Ashizawa K, Okimoto T, Shirafuji T, Kusano H, Ayabe H, Hayashi K. Anterior mediastinal bronchogenic cyst: demonstration of complicating malignancy by CT and MRI. Br J Radiol. 2001. 74:959–961.14. Kumar A, Aggarwal S, Halder S, Kumar S, Khilnani GC. Thoracoscopic excision of mediastinal bronchogenic cyst: a case report and review of literature. Indian J Chest Dis Allied Sci. 2003. 45:199–201.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- X-ray findings of bronchogenic cyst
- A case of congenital intrapulmonalry bronchogenic cyst
- Mediastinal Bronchogenic Cyst Misdiagnosed as Asthma and Dysphagia in a Child: One Case Report
- Anterior Mediastinal Bronchogenic Cysts Manifesting as a Solid Mass: A Report of Three Cases
- Bronchogenic Cyst in Posterior Mediastinum with Butterfly Vertebra: A Case Report
