Surgical management of a failed internal root resorption treatment: a histological and clinical report
- Affiliations
-
- 1Iranian Center for Endodontic Research, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
- 2Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
- 3Department of Craniofacial Biology, School of Dental Medicine, University of Colorado Denver, Aurora, CO, USA. sanam.kheirieh@ucdenver.edu
Abstract
- This article presents the successful surgical management of a failed mineral trioxide aggregate (MTA) orthograde obturation of a tooth with a history of impact trauma and perforated internal root resorption. A symptomatic maxillary lateral incisor with a history of perforation due to internal root resorption and nonsurgical repair using MTA was referred. Unintentional overfill of the defect with MTA had occurred 4 yr before the initial visit. The excess MTA had since disappeared, and a radiolucent lesion adjacent to the perforation site was evident radiographically. Surgical endodontic retreatment was performed using calcium enriched mixture (CEM) cement as a repair material. Histological examination of the lesion revealed granulation tissue with chronic inflammation, and small fragments of MTA encapsulated within fibroconnective tissue. At the one and two year follow up exams, all signs and symptoms of disease had resolved and the tooth was functional. Complete radiographic healing of the lesion was observed two years after the initial visit. This case report illustrates how the selection of an appropriate approach to treatment of a perforation can affect the long term prognosis of a tooth. In addition, extrusion of MTA into a periradicular lesion should be avoided.
Keyword
MeSH Terms
Figure
-

Figure 1 (a) Immediate postoperative periapical x-ray of orthograde MTA perforation repair (- 4 years before the surgical retreatment), extruded MTA was evident; (b) Preoperative periapical x-ray of the lateral incisor tooth shows complete resorption of extruded MTA and a lateral lesion adjacent to perforation site after 4 years; (c) Clinical photograph shows localized inflammation and swelling.
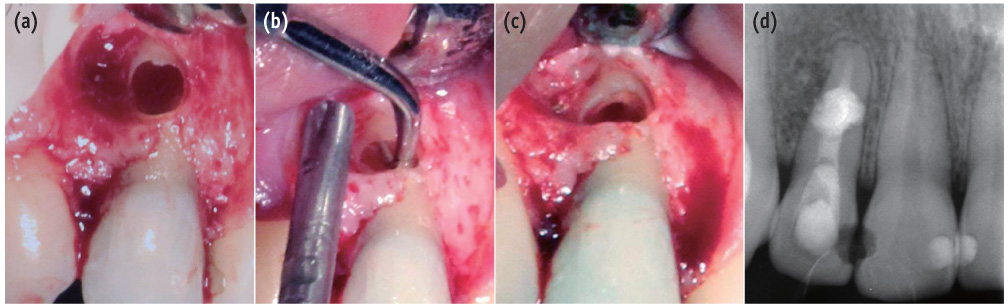
Figure 2 (a) Intra-radicular and bony defect after curettage of the lesion; (b) Using an ultrasonic retrotip in a coronoapical direction the apical portion of root canal was instrumented; (c) The canal was shaped and cleaned; (d) Filling and sealing of the apical portion of the root canal as well as the intra-radicular defect using calcium enriched mixture (CEM) cement was verified radiographically.

Figure 3 (a) Photomicrograph shows granulation tissue with chronic inflammatory cells (H&E staining, Mag. ×200); (b) A macrophage containing phagocyte particles (H&E staining, Mag. ×1,000); (c) A multinucleated giant cell (H&E staining, Mag. ×1,000); (d) Fragments of MTA of different sizes were seen (H&E staining, Mag. ×200); (e) A higher magnification of an MTA fragment which is encapsulated within fibrous connective tissue (H&E staining, Mag. ×1,000).

Figure 4 (a) Clinical photograph shows uninflamed overlying soft tissues; (b) Recall radiograph after one year; (c) Recall radiograph after two years revealed bony healing as well as establishment of PDL.
Reference
-
1. Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. J Endod. 2010; 36:1107–1121.
Article2. Goultschin J, Nitzan D, Azaz B. Root resorption. Review and discussion. Oral Surg Oral Med Oral Pathol. 1982; 54:586–590.3. Nunes E, Silveira FF, Soares JA, Duarte MA, Soares SM. Treatment of perforating internal root resorption with MTA: a case report. J Oral Sci. 2012; 54:127–131.
Article4. Hsien HC, Cheng YA, Lee YL, Lan WH, Lin CP. Repair of perforating internal resorption with mineral trioxide aggregate: a case report. J Endod. 2003; 29:538–539.
Article5. Altundasar E, Demir B. Management of a perforating internal resorptive defect with mineral trioxide aggregate: a case report. J Endod. 2009; 35:1441–1444.
Article6. Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review-part II: leakage and biocompatibility investigations. J Endod. 2010; 36:190–202.
Article7. Noetzel J, Ozer K, Reisshauer BH, Anil A, Rössler R, Neumann K, Kielbassa AM. Tissue responses to an experimental calcium phosphate cement and mineral trioxide aggregate as materials for furcation perforation repair: a histological study in dogs. Clin Oral Investig. 2006; 10:77–83.
Article8. Regan JD, Gutmann JL, Witherspoon DE. Comparison of Diaket and MTA when used as root-end filling materials to support regeneration of the periradicular tissues. Int Endod J. 2002; 35:840–847.
Article9. Asgary S, Eghbal MJ, Parirokh M, Ghoddusi J, Kheirieh S, Brink F. Comparison of mineral trioxide aggregate's composition with Portland cements and a new endodontic cement. J Endod. 2009; 35:243–250.
Article10. Mozayeni MA, Milani AS, Marvasti LA, Asgary S. Cytotoxicity of calcium enriched mixture cement compared with mineral trioxide aggregate and intermediate restorative material. Aust Endod J. 2012; 38:70–75.
Article11. Parirokh M, Mirsoltani B, Raoof M, Tabrizchi H, Haghdoost AA. Comparative study of subcutaneous tissue responses to a novel root-end filling material and white and grey mineral trioxide aggregate. Int Endod J. 2011; 44:283–289.
Article12. Samiee M, Eghbal MJ, Parirokh M, Abbas FM, Asgary S. Repair of furcal perforation using a new endodontic cement. Clin Oral Investig. 2010; 14:653–658.
Article13. Asgary S, Eghbal MJ, Ehsani S. Periradicular regeneration after endodontic surgery with calcium-enriched mixture cement in dogs. J Endod. 2010; 36:837–841.
Article14. Nosrat A, Peimani A, Asgary S. A preliminary report on histological outcome of pulpotomy with endodontic biomaterials vs calcium hydroxide. Restor Dent Endod. 2013; 38:227–233.
Article15. Nosrat A, Asgary S, Eghbal MJ, Ghoddusi J, Bayat-Movahed S. Calcium-enriched mixture cement as artificial apical barrier: a case series. J Conserv Dent. 2011; 14:427–431.
Article16. Asgary S, Nosrat A, Seifi A. Management of inflammatory external root resorption by using calcium-enriched mixture cement: a case report. J Endod. 2011; 37:411–413.
Article17. Ball RL, Barbizam JV, Cohenca N. Intraoperative endodontic applications of cone-beam computed tomography. J Endod. 2013; 39:548–557.
Article18. Nosrat A, Nekoofar MH, Bolhari B, Dummer PM. Unintentional extrusion of mineral trioxide aggregate: a report of three cases. Int Endod J. 2012; 45:1165–1176.
Article19. Saghiri MA, Lotfi M, Saghiri AM, Vosoughhosseini S, Fatemi A, Shiezadeh V, Ranjkesh B. Effect of pH on sealing ability of white mineral trioxide aggregate as a root-end filling material. J Endod. 2008; 34:1226–1229.
Article20. Shokouhinejad N, Nekoofar MH, Iravani A, Kharrazifard MJ, Dummer PM. Effect of acidic environment on the push-out bond strength of mineral trioxide aggregate. J Endod. 2010; 36:871–874.
Article21. Namazikhah MS, Nekoofar MH, Sheykhrezae MS, Salariyeh S, Hayes SJ, Bryant ST, Mohammadi MM, Dummer PM. The effect of pH on surface hardness and microstructure of mineral trioxide aggregate. Int Endod J. 2008; 41:108–116.
Article22. Nekoofar MH, Namazikhah MS, Sheykhrezae MS, Mohammadi MM, Kazemi A, Aseeley Z, Dummer PM. pH of pus collected from periapical abscesses. Int Endod J. 2009; 42:534–538.
Article23. Oloomi K, Saberi E, Mokhtari H, Mokhtari Zonouzi HR, Nosrat A, Nekoofar MH, Dummer PM. Evaluation of the effect of blood contamination on the compressive strength of MTA modified with hydration accelerators. Restor Dent Endod. 2013; 38:128–133.
Article24. Nekoofar MH, Oloomi K, Sheykhrezae MS, Tabor R, Stone DF, Dummer PM. An evaluation of the effect of blood and human serum on the surface microhardness and surface microstructure of mineral trioxide aggregate. Int Endod J. 2010; 43:849–858.
Article25. Chen CL, Huang TH, Ding SJ, Shie MY, Kao CT. Comparison of calcium and silicate cement and mineral trioxide aggregate biologic effects and bone markers expression in MG63 cells. J Endod. 2009; 35:682–685.
Article26. Asgary S, Ehsani S. MTA resorption and periradicular healing in an open-apex incisor: a case report. Saudi Dent J. 2012; 24:55–59.
Article27. Camilleri J. Characterization of hydration products of mineral trioxide aggregate. Int Endod J. 2008; 41:408–417.
Article28. Asgary S, Eghbal MJ, Parirokh M, Ghoddusi J. Effect of two storage solutions on surface topography of two root-end fillings. Aust Endod J. 2009; 35:147–152.
Article29. Reyes-Carmona JF, Felippe MS, Felippe WT. A phosphate-buffered saline intracanal dressing improves the biomineralization ability of mineral trioxide aggregate apical plugs. J Endod. 2010; 36:1648–1652.
Article30. Parirokh M, Askarifard S, Mansouri S, Haghdoost AA, Raoof M, Torabinejad M. Effect of phosphate buffer saline on coronal leakage of mineral trioxide aggregate. J Oral Sci. 2009; 51:187–191.
Article31. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod. 2005; 31:97–100.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A roentgenographic study on apical root resorption of human permanent teeth
- A study on the affecting factors on root resorption
- A radiographic study on root resorption in the malocclusion patients before orthodontic treatment
- Multiple idiopathic external and internal resorption: Case report with cone-beam computed tomography findings
- Pressure Root Resorption of the Second Molar Caused by Third Molar Impaction: A Case Report of Severely Resorbed Root with Vital Pulp
