Korean J Urol.
2013 Jun;54(6):394-398.
Transient Distal Penile Corporoglanular Shunt as an Adjunct to Aspiration and Irrigation Procedures in the Treatment of Early Ischemic Priapism
- Affiliations
-
- 1Urology Clinics, Kartal Training and Research Hospital, Istanbul, Turkey. ocanguven@yahoo.com
Abstract
- PURPOSE
Ischemic priapism, a compartment syndrome, requires urgent treatment in order to nourish the corpora cavernosa. As the first step, aspiration of blood and irrigation of the cavernosal bodies is performed to prevent fibrotic activity and secure erectile capability. During aspiration, there are risks of cardiovascular side effects of adrenergic agonists. We aimed to evaluate a transient distal penile corporoglanular shunt technique in place of aspiration and irrigation techniques for treatment of early ischemic priapism.
MATERIALS AND METHODS
A transient distal penile shunt was applied to 15 patients with early ischemic priapism between January 2011 and May 2012. Priapism duration, history, causes, pain, and any prior management of priapism were assessed in all patients. A complete blood count and penile Doppler ultrasonography were performed, which showed attenuated blood flow in the cavernosal artery. A sterile closed system blood collection set, which has two needles and tubing, was used for the transient distal penile shunt.
RESULTS
Ten of 15 patients with early ischemic priapism were successfully treated with this transient shunt technique. No additional procedures were needed after the resolution of rigidity in the 10 successfully treated patients.
CONCLUSIONS
The transient nature of this technique is an advantage over aspiration and irrigation in the treatment of early ischemic priapism. Our results indicate that the technique can be offered for patients with an ischemic priapism episode of no more than 7 hours.
MeSH Terms
-
Adrenergic Agonists
Arteries
Blood Cell Count
Compartment Syndromes
Humans
Hypogonadism
Imidazoles
Male
Mitochondrial Diseases
Needles
Nitro Compounds
Ophthalmoplegia
Penile Diseases
Penile Erection
Priapism
Resin Cements
Ultrasonography, Doppler
Urologic Surgical Procedures
Adrenergic Agonists
Hypogonadism
Imidazoles
Mitochondrial Diseases
Nitro Compounds
Ophthalmoplegia
Resin Cements
Figure
-

FIG. 1 One of the needles was inserted in the corpus cavernosum and the needle on the other end of the set was inserted in the glans.
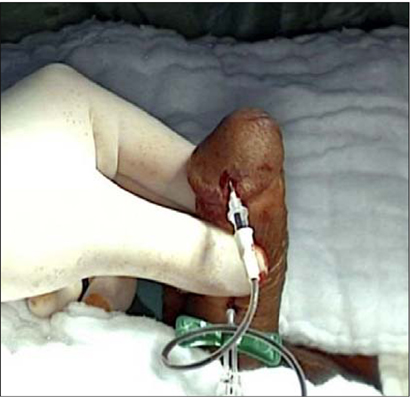
FIG. 2 Corporal bodies were squeezed to increase the pressure inside the corpus cavernosa.
Reference
-
1. Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JP, Lue TF, et al. American Urological Association guideline on the management of priapism. J Urol. 2003; 170(4 Pt 1):1318–1324.2. Berger R, Billups K, Brock G, Broderick GA, Dhabuwala CB, Goldstein I, et al. Report of the American Foundation for Urologic Disease (AFUD) Thought Leader Panel for evaluation and treatment of priapism. Int J Impot Res. 2001; 13:Suppl 5. S39–S43.3. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999; 11:319–326.4. Spycher MA, Hauri D. The ultrastructure of the erectile tissue in priapism. J Urol. 1986; 135:142–147.5. Brant WO, Bella AJ, Gracia MM, Lue TF. Priapism. In : Hohenfellner M, Santucci RA, editors. Emergencies in urology. Heidelberg: Springer;2007. p. 274–289.6. Burnett AL, Pierorazio PM. Corporal "snake" maneuver: corporoglanular shunt surgical modification for ischemic priapism. J Sex Med. 2009; 6:1171–1176.7. Chung SY, Stein RJ, Cannon TW, Nelson JB. Novel technique in the management of low flow priapism. J Urol. 2003; 170:1952.8. Lee M, Cannon B, Sharifi R. Chart for preparation of dilutions of alpha-adrenergic agonists for intracavernous use in treatment of priapism. J Urol. 1995; 153:1182–1183.9. Mantadakis E, Ewalt DH, Cavender JD, Rogers ZR, Buchanan GR. Outpatient penile aspiration and epinephrine irrigation for young patients with sickle cell anemia and prolonged priapism. Blood. 2000; 95:78–82.10. Winter CC. Cure of idiopathic priapism: new procedure for creating fistula between glans penis and corpora cavernosa. Urology. 1976; 8:389–391.11. Ebbehoj J. A new operation for priapism. Scand J Plast Reconstr Surg. 1974; 8:241–242.12. Ercole CJ, Pontes JE, Pierce JM Jr. Changing surgical concepts in the treatment of priapism. J Urol. 1981; 125:210–211.13. Lue TF, Pescatori ES. Distal cavernosum-glans shunts for ischemic priapism. J Sex Med. 2006; 3:749–752.14. Sacher EC, Sayegh E, Frensilli F, Crum P, Akers R. Cavernospongiosum shunt in the treatment of priapism. J Urol. 1972; 108:97–100.15. Grayhack JT, Mccullough W, Oconor VJ Jr, Trıppel O. Venous bypass to control prıapısm. Invest Urol. 1964; 1:509–513.16. Stein RJ, Patel AS, Benoit RM. Treatment of postpriapism erectile dysfunction by closure of persistent distal glans-cavernosum fistulas 5 years after shunt creation. Urology. 2005; 65:592.17. Kirshner A, Davis RR. Priapism associated with the switch from oral to injectable risperidone. J Clin Psychopharmacol. 2006; 26:626–628.18. Chen KK, Chou YH, Chang LS, Chen MT. Sonographic measurement of penile erectile volume. J Clin Ultrasound. 1992; 20:247–253.
